NHS कर्मचारी WiFi: हेल्थकेअरमध्ये सुरक्षित वायरलेस नेटवर्क्स कसे तैनात करावे
हे तांत्रिक संदर्भ मार्गदर्शक NHS कर्मचारी WiFi साठी आर्किटेक्चर, सुरक्षा प्रोटोकॉल्स आणि डिप्लॉयमेंट धोरणांचे तपशील देते, ज्यामध्ये 802.1X ऑथेंटिकेशन, VLAN सेगमेंटेशन, BYOD धोरणे आणि DSP टूलकिट अनुपालन समाविष्ट आहे. हे IT लीडर्सना एंटरप्राइझ-ग्रेड वायरलेस नेटवर्क्स तैनात करण्यासाठी कृती करण्यायोग्य मार्गदर्शन प्रदान करते जे सुरक्षेशी तडजोड न करता सामायिक भौतिक पायाभूत सुविधांवर क्लिनिकल, प्रशासकीय आणि अतिथी वापरकर्त्यांना सेवा देतात. तुम्ही नवीन डिप्लॉयमेंटची योजना आखत असाल किंवा विद्यमान इस्टेट मजबूत करत असाल, हे मार्गदर्शक या तिमाहीत कार्य करण्यासाठी आवश्यक असलेले निर्णय फ्रेमवर्क्स आणि अंमलबजावणीचे टप्पे प्रदान करते.
हे मार्गदर्शक ऐका
पॉडकास्ट ट्रान्सक्रिप्ट पहा
📚 आमच्या मुख्य मालिकेचा भाग: Enterprise WiFi Security Guide →

कार्यकारी सारांश
NHS संपत्तियों में सुरक्षित, विश्वसनीय WiFi तैनात करना अब कोई वैकल्पिक सुविधा नहीं है — यह एक महत्वपूर्ण नैदानिक बुनियादी ढांचा (clinical infrastructure) है। मोबाइल-फर्स्ट रोगी देखभाल, इलेक्ट्रॉनिक स्वास्थ्य रिकॉर्ड (EHR), और जुड़े हुए चिकित्सा उपकरणों की ओर बढ़ता झुकाव एक ऐसे वायरलेस आर्किटेक्चर की मांग करता है जो कड़े सुरक्षा नियंत्रणों के साथ निर्बाध रोमिंग को संतुलित करे।
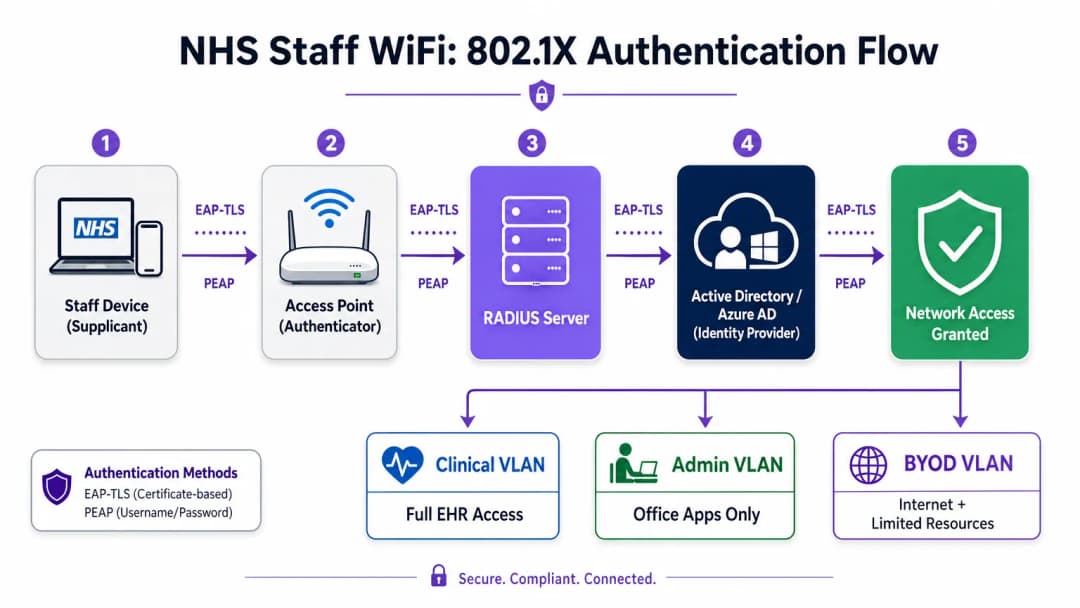
IT प्रबंधकों, नेटवर्क आर्किटेक्ट्स और CTOs के लिए, मुख्य चुनौती सुरक्षा से समझौता किए बिना साझा भौतिक बुनियादी ढांचे पर विभिन्न उपयोगकर्ता समूहों — नैदानिक कर्मचारियों, प्रशासनिक कर्मियों, रोगियों और मेहमानों — को समायोजित करना है, जो NHS डेटा सुरक्षा और संरक्षण (DSP) टूलकिट आवश्यकताओं को पूरा करता हो। यह मार्गदर्शिका NHS स्टाफ WiFi के लिए तकनीकी आवश्यकताओं का विवरण देती है, जिसमें IEEE 802.1X जैसे मजबूत प्रमाणीकरण ढांचे, VLANs के माध्यम से तार्किक नेटवर्क विभाजन (logical network segmentation), और Bring Your Own Device (BYOD) एंडपॉइंट्स के सुरक्षित ऑनबोर्डिंग पर ध्यान केंद्रित किया गया है।
विरासत (legacy) प्री-शेयर्ड कीज़ (PSK) से दूर जाकर और पहचान-संचालित एक्सेस नीतियों को अपनाकर, स्वास्थ्य सेवा संगठन उल्लंघन के जोखिम को कम कर सकते हैं, परिचालन संबंधी बाधाओं को कम कर सकते हैं, और डिजिटल परिवर्तन कार्यक्रमों के लिए वायरलेस आधार प्रदान कर सकते हैं। इसका व्यावसायिक पक्ष भी उतना ही मजबूत है: हेल्पडेस्क ओवरहेड में कमी, प्रमाणित DSP टूलकिट अनुपालन, और एक ऐसा नेटवर्क जो बिना किसी पूर्ण बुनियादी ढांचे के पुनर्निर्माण के भविष्य के नैदानिक नवाचारों का समर्थन करने में सक्षम हो।
तकनीकी गहन विश्लेषण
प्रमाणीकरण और एक्सेस नियंत्रण
एक सुरक्षित स्वास्थ्य सेवा वायरलेस नेटवर्क की नींव पहचान-आधारित एक्सेस नियंत्रण है। प्री-शेयर्ड कीज़ का उपयोग करने वाले विरासत WPA2-Personal नेटवर्क नैदानिक वातावरण के लिए मौलिक रूप से अनुपयुक्त हैं। वे कोई व्यक्तिगत जवाबदेही प्रदान नहीं करते हैं, कर्मचारियों के जाने पर ऑनबोर्डिंग हटाने की प्रक्रिया को जटिल बनाते हैं, और क्रेडेंशियल के साथ समझौता होने या इच्छित समूह से बाहर साझा किए जाने पर विफलता का एक एकल बिंदु (single point of failure) पेश करते हैं।
आधुनिक NHS तैनाती में WPA3-Enterprise (या न्यूनतम संक्रमण स्थिति के रूप में WPA2-Enterprise) को IEEE 802.1X प्रमाणीकरण का उपयोग करके अनिवार्य किया जाना चाहिए। इस ढांचे के लिए आवश्यक है कि नेटवर्क एक्सेस दिए जाने से पहले प्रत्येक उपयोगकर्ता या डिवाइस अद्वितीय क्रेडेंशियल प्रस्तुत करे, और उस प्रमाणीकरण का परिणाम यह निर्धारित करता है कि डिवाइस को किस तार्किक नेटवर्क सेगमेंट पर रखा जाए।
स्वास्थ्य सेवा तैनाती में दो EAP तरीके हावी हैं:
| EAP तरीका | प्रमाणीकरण तंत्र | इसके लिए सबसे उपयुक्त | सुरक्षा स्तर |
|---|---|---|---|
| EAP-TLS | क्लाइंट-साइड डिजिटल प्रमाणपत्र | कॉर्पोरेट-प्रबंधित नैदानिक उपकरण | उच्चतम — फ़िशिंग के लिए कोई पासवर्ड नहीं |
| PEAP-MSCHAPv2 | एन्क्रिप्टेड टनल में उपयोगकर्ता नाम/पासवर्ड | BYOD, व्यवस्थापक कर्मचारी, विरासत उपकरण | उच्च — TLS द्वारा सुरक्षित क्रेडेंशियल |
EAP-TLS कॉर्पोरेट उपकरणों के लिए स्वर्ण मानक (gold standard) है। प्रमाणपत्रों को मोबाइल डिवाइस मैनेजमेंट (MDM) प्लेटफॉर्म के माध्यम से वितरित किया जाता है, जिससे ज़ीरो-टच प्रमाणीकरण सक्षम होता है — डिवाइस पृष्ठभूमि में चुपचाप प्रमाणित हो जाता है। PEAP-MSCHAPv2 एक एन्क्रिप्टेड TLS सत्र के भीतर एक्टिव डायरेक्ट्री या एज़्योर AD क्रेडेंशियल को सुरक्षित रूप से टनल करता है, जिससे यह BYOD परिदृश्यों के लिए उपयुक्त हो जाता है जहां प्रमाणपत्र प्रबंधन व्यावहारिक नहीं है।
वायरलेस बुनियादी ढांचे को संगठन के केंद्रीय पहचान प्रदाता (IdP) के साथ एकीकृत करना यह सुनिश्चित करता है कि किसी कर्मचारी का AD खाता अक्षम होने पर एक्सेस स्वचालित रूप से रद्द हो जाए, जो सीधे एक्सेस लाइफसाइकल प्रबंधन के लिए DSP टूलकिट आवश्यकताओं को पूरा करता है।
नेटवर्क विभाजन और ट्रस्ट ज़ोन
भौतिक एक्सेस पॉइंट पूरे अस्पताल के फर्श पर प्रसारण करते हैं, लेकिन तार्किक विभाजन यह सुनिश्चित करता है कि न्यूनतम विशेषाधिकार के सिद्धांत के आधार पर ट्रैफ़िक अलग रहे। स्वास्थ्य सेवा सेटिंग में एक फ्लैट नेटवर्क आर्किटेक्चर एक गंभीर सुरक्षा भेद्यता है, जो एक समझौता किए गए अतिथि डिवाइस या कमजोर IoT सेंसर को संभावित रूप से नैदानिक प्रणालियों तक पहुँचने की अनुमति देता है।
सर्वोत्तम अभ्यास विशिष्ट SSIDs के लिए मैप किए गए अलग वर्चुअल लोकल एरिया नेटवर्क (VLANs) बनाने का निर्देश देता है, जिसमें फ़ायरवॉल नियम उनके बीच ट्रैफ़िक सीमाओं को लागू करते हैं:
| ज़ोन | SSID | प्रमाणीकरण | एक्सेस | QoS प्राथमिकता |
|---|---|---|---|---|
| नैदानिक | NHS-Clinical | EAP-TLS (प्रमाणपत्र) | EHR, PACS, नैदानिक संदेश सेवा | उच्चतम |
| प्रशासनिक | NHS-Staff | PEAP (AD क्रेडेंशियल) | ऑफिस ऐप्स, इंटरनेट | मध्यम |
| मेडिकल IoT | Hidden/MAB | MAC Authentication Bypass | केवल डिवाइस कंट्रोलर | उच्च |
| अतिथि / रोगी | NHS-Guest | Captive Portal | केवल इंटरनेट | निम्न |
| BYOD | NHS-BYOD | PEAP (AD क्रेडेंशियल) | इंटरनेट, सीमित VDI | निम्न |
मेडिकल IoT VLAN विशेष ध्यान देने योग्य है। कई जुड़े हुए चिकित्सा उपकरण — इन्फ्यूजन पंप, रोगी मॉनिटर, वायरलेस कॉल सिस्टम — 802.1X का समर्थन नहीं कर सकते हैं। MAC Authentication Bypass (MAB) इसका विकल्प है, लेकिन इसे सख्त फ़ायरवॉल एक्सेस कंट्रोल लिस्ट (ACLs) के साथ जोड़ा जाना चाहिए जो इन उपकरणों को केवल उनके निर्दिष्ट प्रबंधन सर्वर के साथ संचार करने तक सीमित करते हैं।
BYOD की चुनौती
Bring Your Own Device नीतियां प्रशासनिक कर्मचारियों और आने वाले चिकित्सकों के लिए तेजी से आम हो रही हैं। हालांकि, अप्रबंधित व्यक्तिगत उपकरण एक महत्वपूर्ण जोखिम का प्रतिनिधित्व करते हैं यदि उन्हें विश्वसनीय नेटवर्क सेगमेंट पर जाने की अनुमति दी जाती है।
एक सुरक्षित BYOD तैनाती में इन उपकरणों को एक समर्पित BYOD VLAN पर ऑनबोर्ड करना शामिल है। यह ज़ोन इंटरनेट एक्सेस प्रदान करता है और शायद एक सुरक्षित गेटवे या वर्चुअल डेस्कटॉप इंफ्रास्ट्रक्चर (VDI) के माध्यम से विशिष्ट, गैर-संवेदनशील आंतरिक संसाधनों तक सीमित पहुंच प्रदान करता है। इसमें नैदानिक प्रणालियों या रोगी डेटा स्टोर के लिए सीधे रूटिंग की अनुमति बिल्कुल नहीं होनी चाहिए।

कार्यान्वयन मार्गदर्शिका
एक सुरक्षित NHS स्टाफ WiFi आर्किटेक्चर को तैनात करने के लिए चल रहे नैदानिक संचालन में व्यवधान को कम करने के लिए चरणबद्ध दृष्टिकोण की आवश्यकता होती है।
चरण 1: मूल्यांकन और डिज़ाइन
एक व्यापक वायरलेस साइट सर्वेक्षण के साथ शुरुआत करें। लीड-लाइनेड दीवारों, भारी मशीनरी और घनी आबादी के कारण स्वास्थ्य सेवा वातावरण रेडियो फ्रीक्वेंसी (RF) प्रसार के लिए कुख्यात रूप से कठिन हैं। डिज़ाइन में केवल कवरेज ही नहीं, बल्कि क्षमता का भी ध्यान रखा जाना चाहिए, जिससे आपातकालीन विभागों और बाह्य रोगी क्लीनिकों जैसे उच्च-यातायात वाले क्षेत्रों में पर्याप्त एक्सेस पॉइंट घनत्व सुनिश्चित हो सके।
आवश्यक SSIDs को परिभाषित करें और उन्हें संबंधित VLANs और सुरक्षा नीतियों से मैप करें। प्रसारण SSIDs की संख्या को न्यूनतम रखें — आदर्श रूप से चार से अधिक नहीं — ताकि प्रबंधन ओवरहेड को कम किया जा सके और बीकन फ्रेम कंजेशन को कम किया जा सके, जो समग्र नेटवर्क प्रदर्शन को कम करता है।
चरण 2: बुनियादी ढांचा कॉन्फ़िगरेशन
परिभाषित VLANs का समर्थन करने के लिए कोर स्विचिंग और रूटिंग बुनियादी ढांचे को कॉन्फ़िगर करें। न्यूनतम विशेषाधिकार लागू करने के लिए सेगमेंट के बीच की सीमाओं पर फ़ायरवॉल नियम लागू करें। RADIUS सर्वर (जैसे, Cisco ISE, Aruba ClearPass, या क्लाउड-आधारित RADIUS-as-a-Service) सेट करें और इसे केंद्रीय पहचान प्रदाता के साथ एकीकृत करें। जिन वातावरणों में Purple का प्लेटफ़ॉर्म तैनात है, वहां इस चरण में WiFi Analytics को एकीकृत करना नेटवर्क उपयोग, रोमिंग पैटर्न और क्षमता हॉटस्पॉट में दृश्यता प्रदान करता है।
चरण 3: नीति प्रवर्तन और ऑनबोर्डिंग
प्रमाणीकरण नीतियां तैनात करें। कॉर्पोरेट उपकरणों के लिए, आवश्यक वायरलेस प्रोफाइल और क्लाइंट प्रमाणपत्र (EAP-TLS के लिए) भेजने के लिए MDM समाधान का उपयोग करें। यह सुनिश्चित करता है कि प्रबंधित उपकरण उपयोगकर्ता के हस्तक्षेप के बिना स्वचालित रूप से और सुरक्षित रूप से कनेक्ट हों।
BYOD के लिए, एक स्पष्ट ऑनबोर्डिंग वर्कफ़्लो स्थापित करें — आमतौर पर एक ऑनबोर्डिंग पोर्टल जो उपयोगकर्ता को उनके कॉर्पोरेट क्रेडेंशियल के साथ प्रमाणित करने, स्वीकार्य उपयोग नीति को स्वीकार करने और डिवाइस को सुरक्षित BYOD VLAN पर ले जाने के माध्यम से मार्गदर्शन करता है। Purple के Guest WiFi प्लेटफ़ॉर्म को रोगी और अतिथि SSID के लिए Captive Portal परत के रूप में तैनात किया जा सकता है, जो बड़े पैमाने पर GDPR-अनुरूप डेटा कैप्चर और शर्तों की स्वीकृति को संभालता है।
चरण 4: परीक्षण और सत्यापन
गो-लाइव से पहले, प्रत्येक प्रमाणीकरण पथ, VLAN असाइनमेंट और फ़ायरवॉल नियम का एंड-टू-एंड परीक्षण करें। विशेष रूप से पुनः प्रमाणीकरण घटनाओं की निगरानी करते हुए एक परीक्षण डिवाइस के साथ नैदानिक फर्श पर चलकर रोमिंग व्यवहार को मान्य करें। पुष्टि करें कि फास्ट रोमिंग प्रोटोकॉल (802.11r और 802.11k) सही ढंग से काम कर रहे हैं और एप्लिकेशन सत्र AP संक्रमणों के बाद भी बने रहते हैं।
सर्वोत्तम अभ्यास
प्री-शेयर्ड कीज़ को समाप्त करें। व्यक्तिगत जवाबदेही और केंद्रीकृत एक्सेस नियंत्रण सुनिश्चित करने के लिए सभी कर्मचारियों और नैदानिक नेटवर्क को 802.1X प्रमाणीकरण पर स्थानांतरित करें। यह DSP टूलकिट अनुपालन के लिए एक गैर-परक्राम्य आवश्यकता है।
सख्त विभाजन लागू करें। अतिथि, BYOD, या IoT ट्रैफ़िक को कभी भी नैदानिक डेटा के समान तार्किक सेगमेंट पर अनुमति न दें। डिफ़ॉल्ट नीति के रूप में स्पष्ट अस्वीकार (deny) नियमों के साथ, इंटर-VLAN रूटिंग को नियंत्रित करने के लिए स्टेटफुल फ़ायरवॉल का उपयोग करें।
नैदानिक ट्रैफ़िक को प्राथमिकता दें। विशेष रूप से उच्च भीड़ की अवधि के दौरान, अतिथि या प्रशासनिक ट्रैफ़िक की तुलना में नैदानिक अनुप्रयोगों — वॉयस ओवर WLAN, EHR एक्सेस — को प्राथमिकता देने के लिए वायरलेस कंट्रोलर और स्विच पर QoS नीतियां लागू करें।
फास्ट रोमिंग सक्षम करें। 802.11r (फास्ट BSS ट्रांज़िशन) और 802.11k (रेडियो रिसोर्स मेजरमेंट) को तैनात करें ताकि यह सुनिश्चित हो सके कि नैदानिक कर्मचारी एप्लिकेशन टाइमआउट या टूटे हुए कनेक्शन का अनुभव किए बिना सुविधा के माध्यम से आगे बढ़ सकें।
निरंतर निगरानी। नेटवर्क स्वास्थ्य की निगरानी करने, अनधिकृत एक्सेस पॉइंट की पहचान करने और उपयोगकर्ता रोमिंग व्यवहार को ट्रैक करने के लिए एनालिटिक्स प्लेटफॉर्म का उपयोग करें। फुटफॉल और उपयोग के पैटर्न को समझना — Retail और Hospitality वातावरण में सिद्ध एक तकनीक — क्षमता योजना और समस्या निवारण के लिए अस्पताल की सेटिंग में भी उतनी ही मूल्यवान है।
नियमित ऑडिटिंग। जहां लागू हो, DSP टूलकिट, साइबर एसेंशियल प्लस और ISO 27001 के साथ निरंतर अनुपालन सुनिश्चित करने के लिए वार्षिक वायरलेस जोखिम मूल्यांकन आयोजित करें।
समस्या निवारण और जोखिम शमन
प्रमाणीकरण टाइमआउट
उच्च क्लाइंट घनत्व वाले वातावरण में, RADIUS सर्वर अभिभूत हो सकते हैं, जिससे प्रमाणीकरण टाइमआउट और टूटे हुए कनेक्शन हो सकते हैं। सुनिश्चित करें कि RADIUS बुनियादी ढांचा पर्याप्त रूप से स्केल किया गया है और अत्यधिक उपलब्ध है। कई प्रमाणीकरण सर्वरों में लोड बैलेंसिंग लागू करें और एक प्रमुख परिचालन मीट्रिक के रूप में RADIUS प्रतिक्रिया समय की निगरानी करें।
रोमिंग के मुद्दे
वार्डों के बीच तेजी से चलने वाले नैदानिक कर्मचारियों को टूटे हुए कनेक्शन का अनुभव हो सकता है यदि वायरलेस बुनियादी ढांचा फास्ट रोमिंग प्रोटोकॉल का समर्थन नहीं करता है। वायरलेस कंट्रोलर पर 802.11r और 802.11k सक्षम करें और सुनिश्चित करें कि क्लाइंट डिवाइस इन मानकों का समर्थन करते हैं। कवरेज अंतराल या 'स्टिकी क्लाइंट' मुद्दों की पहचान करने और उन्हें हल करने के लिए पोस्ट-डिप्लॉयमेंट रोमिंग सर्वेक्षण आयोजित करें, जहां एक डिवाइस करीब जाने के बजाय दूर के, कमजोर AP से चिपका रहता है।
विरासत डिवाइस असंगतता
पुराने चिकित्सा उपकरण WPA3 या 802.1X जैसे आधुनिक सुरक्षा प्रोटोकॉल का समर्थन नहीं कर सकते हैं। MAB का उपयोग करके इन उपकरणों को एक समर्पित IoT VLAN पर अलग करें। उनके संचार को केवल आवश्यक प्रबंधन सर्वर तक सीमित करने के लिए सख्त फ़ायरवॉल नियम लागू करें। उन महत्वपूर्ण उपकरणों के लिए हार्डवेयर अपग्रेड या वायरलेस ब्रिज पर विचार करें जिन्हें मूल रूप से सुरक्षित नहीं किया जा सकता है।
प्रमाणपत्र की समाप्ति
EAP-TLS तैनाती परिभाषित समाप्ति अवधि वाले प्रमाणपत्रों पर निर्भर करती है। यदि प्रमाणपत्र नवीनीकरण के बिना समाप्त हो जाते हैं, तो डिवाइस प्रमाणित करने में विफल हो जाएंगे, जिससे व्यापक नैदानिक व्यवधान होगा। MDM प्लेटफॉर्म के माध्यम से SCEP (सिंपल सर्टिफिकेट एनरोलमेंट प्रोटोकॉल) के माध्यम से स्वचालित प्रमाणपत्र नवीनीकरण लागू करें, और सक्रिय रूप से प्रमाणपत्र समाप्ति तिथियों की निगरानी करें।
ROI और व्यावसायिक प्रभाव
एक सुरक्षित, एंटरप्राइज़-ग्रेड वायरलेस आर्किटेक्चर में निवेश नैदानिक, परिचालन और IT डोमेन में मापने योग्य रिटर्न प्रदान करता है।
नैदानिक दक्षता। विश्वसनीय कनेक्टिविटी यह सुनिश्चित करती है कि चिकित्सकों के पास देखभाल के बिंदु पर रोगी के रिकॉर्ड तक तत्काल पहुंच हो, जिससे जानकारी खोजने या टूटे हुए कनेक्शन से निपटने में लगने वाला समय कम हो जाता है। यह सीधे रोगी थ्रूपुट और देखभाल वितरण की गुणवत्ता को प्रभावित करता है।
कम IT ओवरहेड। साझा पासवर्ड और मैन्युअल ऑनबोर्डिंग से हटकर स्वचालित, प्रमाणपत्र-आधारित प्रमाणीकरण की ओर बढ़ने से पासवर्ड रीसेट और कनेक्टिविटी समस्याओं से संबंधित हेल्पडेस्क टिकटों में काफी कमी आती है। एक NHS ट्रस्ट ने 802.1X पर माइग्रेशन के बाद वायरलेस से संबंधित हेल्पडेस्क कॉल में 40% की कमी दर्ज की।
जोखिम शमन। सख्त विभाजन और मजबूत प्रमाणीकरण DSP टूलकिट आवश्यकताओं को पूरा करने, डेटा उल्लंघनों या अनुपालन विफलताओं से जुड़े वित्तीय और प्रतिष्ठित जोखिमों को कम करने के लिए मौलिक हैं। डेटा उल्लंघन की लागत उचित रूप से तैयार की गई वायरलेस संपत्ति में निवेश से कहीं अधिक है।
भविष्य के लिए तैयार करना (Future-Proofing)। एक अच्छी तरह से डिज़ाइन किया गया वायरलेस नेटवर्क भविष्य की डिजिटल स्वास्थ्य पहलों — स्थान-आधारित सेवाएं, रीयल-टाइम एसेट ट्रैकिंग, उन्नत टेलीहेल्थ एप्लिकेशन — के लिए आधार प्रदान करता है, जो Healthcare और Transport जैसे संबंधित क्षेत्रों में व्यापक रणनीतिक लक्ष्यों के साथ संरेखित होता है जहां मोबाइल कनेक्टिविटी परिचालन दक्षता को रेखांकित करती है।
उन संगठनों के लिए जो यह समझना चाहते हैं कि Purple का प्लेटफ़ॉर्म इस आर्किटेक्चर के अतिथि और रोगी WiFi परत से कैसे मेल खाता है, Healthcare उद्योग पृष्ठ NHS-संगत Captive Portal, एनालिटिक्स और GDPR-अनुरूप डेटा हैंडलिंग क्षमताओं का एक विस्तृत अवलोकन प्रदान करता है। वही एनालिटिक्स सिद्धांत जो Retail में ग्राहक जुड़ाव को बढ़ावा देते हैं, सीधे अस्पताल संपदा टीमों के लिए परिचालन खुफिया में अनुवादित होते हैं।
महत्वाच्या व्याख्या
IEEE 802.1X
पोर्ट-आधारित नेटवर्क ॲक्सेस कंट्रोल (PNAC) साठी एक IEEE मानक. हे LAN किंवा WLAN शी कनेक्ट होऊ इच्छिणाऱ्या उपकरणांना ऑथेंटिकेशन यंत्रणा प्रदान करते, ज्यामध्ये ॲक्सेस देण्यापूर्वी प्रत्येक उपकरणाला क्रेडेंशियल्स सादर करणे आवश्यक असते.
कर्मचारी आणि क्लिनिकल उपकरणांसाठी असुरक्षित शेअर्ड पासवर्ड्सच्या जागी वैयक्तिक, आयडेंटिटी-आधारित लॉगिन्स आणण्यासाठी हे अनिवार्य मानक आहे. हा DSP टूलकिट-सुसंगत वायरलेस आर्किटेक्चरचा आधारस्तंभ आहे.
VLAN (Virtual Local Area Network)
एक लॉजिकल सबनेटवर्क जे वेगवेगळ्या फिजिकल नेटवर्क सेगमेंट्समधील उपकरणांचा समूह एकत्र करते. VLANs नेटवर्क ॲडमिनिस्ट्रेटर्सना विविध वापरकर्ता गटांच्या कार्यात्मक आणि सुरक्षा आवश्यकतांशी जुळण्यासाठी सिंगल स्विच्ड नेटवर्कचे विभाजन करण्याची परवानगी देतात.
क्लिनिकल ट्रॅफिकला अतिथी आणि प्रशासकीय ट्रॅफिकपासून वेगळे करण्यासाठी, संभाव्य सुरक्षा उल्लंघनाचा ब्लास्ट रेडियस मर्यादित करण्यासाठी आणि किमान विशेषाधिकाराचे तत्त्व लागू करण्यासाठी VLANs आवश्यक आहेत.
RADIUS (Remote Authentication Dial-In User Service)
एक नेटवर्किंग प्रोटोकॉल जो नेटवर्क सेवेशी कनेक्ट होणाऱ्या आणि वापरणाऱ्या वापरकर्त्यांसाठी सेंट्रलाइज्ड ऑथेंटिकेशन, ऑथोरायझेशन आणि अकाउंटिंग (AAA) मॅनेजमेंट प्रदान करतो.
RADIUS सर्व्हर वायरलेस ॲक्सेस पॉइंट्स आणि सेंट्रल आयडेंटिटी डेटाबेस (ॲक्टिव्ह डिरेक्टरी) यांच्यातील निर्णय इंजिन म्हणून कार्य करतो, कोणाला ॲक्सेस मिळेल आणि त्यांना कोणत्या VLAN वर नियुक्त केले जाईल हे ठरवतो.
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
एक EAP पद्धत जी सुरक्षित, परस्पर ऑथेंटिकेटेड कनेक्शन स्थापित करण्यासाठी क्लायंट आणि सर्व्हर सर्टिफिकेट्सवर अवलंबून असते. वैध सर्टिफिकेटशिवाय कोणताही पक्ष दुसऱ्यावर विश्वास ठेवत नाही.
हॉस्पिटलच्या मालकीच्या उपकरणांना ऑथेंटिकेट करण्यासाठी सर्वात सुरक्षित पद्धत. MDM द्वारे वितरित केलेली सर्टिफिकेट्स हे सुनिश्चित करतात की केवळ मॅनेज्ड, ट्रस्टेड एंडपॉइंट्स क्लिनिकल नेटवर्कमध्ये प्रवेश करू शकतात, ज्यामध्ये फिशिंग किंवा शेअर करण्यासाठी कोणताही पासवर्ड नसतो.
MAB (MAC Authentication Bypass)
उपकरणांच्या हार्डवेअर MAC ॲड्रेसवर आधारित त्यांना ऑथेंटिकेट करण्याची एक पद्धत, जी 802.1X ला सपोर्ट न करणाऱ्या उपकरणांसाठी फॉलबॅक म्हणून वापरली जाते.
लेगसी वैद्यकीय IoT उपकरणांसाठी आवश्यक आहे ज्यांना नेटवर्क ॲक्सेसची आवश्यकता आहे परंतु ते जटिल ऑथेंटिकेशन प्रोटोकॉल्स हाताळू शकत नाहीत. उपकरणाला त्याच्या परवानगी असलेल्या कम्युनिकेशन मार्गांवर मर्यादित ठेवण्यासाठी नेहमी कठोर फायरवॉल ACLs सोबत जोडले जाणे आवश्यक आहे.
DSP Toolkit (Data Security and Protection Toolkit)
NHS इंग्लंडने अनिवार्य केलेले एक ऑनलाइन सेल्फ-असेसमेंट टूल जे NHS पेशंट डेटा आणि सिस्टीम्समध्ये ॲक्सेस असलेल्या सर्व संस्थांनी पूर्ण करणे आवश्यक आहे. हे नॅशनल डेटा गार्डियनच्या दहा डेटा सुरक्षा मानकांशी मॅप करते.
NHS संस्था आणि त्यांच्या पुरवठादारांसाठी DSP टूलकिटचे अनुपालन अनिवार्य आहे. मजबूत वायरलेस सुरक्षा — ज्यामध्ये 802.1X, सेगमेंटेशन आणि ॲक्सेस लाइफसायकल मॅनेजमेंट समाविष्ट आहे — अनुपालन प्रदर्शित करण्याचा एक महत्त्वपूर्ण घटक आहे.
SSID (Service Set Identifier)
802.11 वायरलेस लोकल एरिया नेटवर्कशी संबंधित प्राथमिक नाव, जे क्लायंट उपकरणांना नेटवर्क ओळखण्यासाठी आणि कनेक्ट करण्यासाठी ॲक्सेस पॉइंट्सद्वारे ब्रॉडकास्ट केले जाते.
हॉस्पिटल्सनी मॅनेजमेंट ओव्हरहेड आणि RF ओव्हरहेड कमी करण्यासाठी ब्रॉडकास्ट SSIDs (उदा., NHS-Clinical, NHS-Guest) ची संख्या कमीत कमी ठेवली पाहिजे. प्रत्येक SSID विशिष्ट सुरक्षा धोरण आणि VLAN शी मॅप केलेला असावा.
QoS (Quality of Service)
असे तंत्रज्ञान जे नेटवर्कवरील पॅकेट लॉस, लेटन्सी आणि जिटर कमी करण्यासाठी डेटा ट्रॅफिक व्यवस्थापित करते आणि विशिष्ट प्रकारच्या ट्रॅफिकला इतरांपेक्षा प्राधान्य देते.
हेल्थकेअरमध्ये हे सुनिश्चित करण्यासाठी महत्त्वपूर्ण आहे की लाइफ-क्रिटिकल क्लिनिकल ॲप्लिकेशन्स आणि व्हॉइस कम्युनिकेशन्सना नेहमी अतिथी व्हिडिओ स्ट्रीमिंग किंवा सॉफ्टवेअर अपडेट्स सारख्या कमी महत्त्वाच्या ट्रॅफिकपेक्षा प्राधान्य दिले जाते.
802.11r (Fast BSS Transition)
एक IEEE सुधारणा जी फिजिकल ट्रान्झिशन होण्यापूर्वी क्लायंटला टार्गेट AP वर प्री-ऑथेंटिकेट करून ॲक्सेस पॉइंट्स दरम्यान फास्ट रोमिंग सक्षम करते, ज्यामुळे रोमिंग लेटन्सी लक्षणीयरीत्या कमी होते.
क्लिनिकल वातावरणासाठी आवश्यक आहे जिथे कर्मचारी सतत फिरत असतात. 802.11r शिवाय, उपकरणांना प्रत्येक AP ट्रान्झिशनवर पूर्ण RADIUS री-ऑथेंटिकेशन करावे लागते, ज्यामुळे ॲप्लिकेशन सेशन्स टाइम आउट होऊ शकतात.
सोडवलेली उदाहरणे
एक NHS ट्रस्ट अनेक वॉर्ड्समध्ये नवीन मोबाइल वर्कस्टेशन्स (Workstations on Wheels) तैनात करत आहे. नर्सेस ॲक्सेस पॉइंट्स दरम्यान फिरत असताना या उपकरणांची कनेक्टिव्हिटी टिकून राहील याची खात्री IT टीमला करायची आहे, तसेच इलेक्ट्रॉनिक हेल्थ रेकॉर्ड सिस्टीम असलेल्या क्लिनिकल VLAN मध्ये फक्त अधिकृत उपकरणांनाच प्रवेश मिळेल याची हमी द्यायची आहे.
ट्रस्टने EAP-TLS वापरून 802.1X ऑथेंटिकेशन फ्रेमवर्क लागू केले पाहिजे. IT टीम त्यांच्या MDM सोल्यूशनचा वापर करून प्रत्येक वर्कस्टेशनला एक युनिक क्लायंट सर्टिफिकेट आणि संबंधित वायरलेस प्रोफाइल पुश करेल. वायरलेस कंट्रोलर्स या उपकरणांना RADIUS सर्व्हरच्या विरूद्ध ऑथेंटिकेट करण्यासाठी कॉन्फिगर केले जातील, जे अंतर्गत PKI च्या विरूद्ध सर्टिफिकेटची पडताळणी करते. यशस्वी ऑथेंटिकेशनवर, RADIUS सर्व्हर डायनॅमिकली वर्कस्टेशनला RADIUS ॲट्रिब्युट (उदा., Tunnel-Private-Group-ID) द्वारे समर्पित क्लिनिकल VLAN वर नियुक्त करतो. रोमिंगची आवश्यकता पूर्ण करण्यासाठी, वायरलेस इन्फ्रास्ट्रक्चरवर 802.11r (Fast BSS Transition) आणि 802.11k (Radio Resource Measurement) सक्षम केले जाणे आवश्यक आहे जेणेकरून वर्कस्टेशन्सना प्रत्येक वेळी RADIUS सर्व्हरच्या विरूद्ध पूर्ण री-ऑथेंटिकेशन सायकल न करता ॲक्सेस पॉइंट्स दरम्यान अखंडपणे ट्रान्झिशन करता येईल.
एका हॉस्पिटलला त्यांच्या वैयक्तिक लॅपटॉप्स (BYOD) वापरून भेट देणाऱ्या लोकॅम डॉक्टरांसाठी इंटरनेट ॲक्सेस प्रदान करणे आवश्यक आहे. या डॉक्टरांना क्लाउड-आधारित वैद्यकीय संदर्भ साधनांमध्ये प्रवेश करणे आवश्यक आहे परंतु त्यांना हॉस्पिटलच्या अंतर्गत पेशंट डेटाबेसमध्ये प्रवेश करण्यास सक्त मनाई असली पाहिजे.
हॉस्पिटलने आयसोलेटेड BYOD VLAN शी मॅप केलेला समर्पित BYOD SSID तैनात केला पाहिजे. ऑथेंटिकेशन PEAP-MSCHAPv2 वापरून 802.1X द्वारे हाताळले जावे, ज्यामुळे लोकॅम्सना आगमनावर HR द्वारे प्रदान केलेल्या तात्पुरत्या ॲक्टिव्ह डिरेक्टरी क्रेडेंशियल्सचा वापर करून लॉग इन करता येईल. कोर फायरवॉल एका ACL सह कॉन्फिगर केले जाणे आवश्यक आहे जे BYOD VLAN वरून क्लिनिकल किंवा प्रशासकीय VLANs कडे कोणत्याही राउटिंगला स्पष्टपणे नाकारते, केवळ इंटरनेटवरील आउटबाउंड ट्रॅफिकला परवानगी देते. याव्यतिरिक्त, पूर्ण इंटरनेट ॲक्सेस देण्यापूर्वी ॲक्सेप्टेबल युज पॉलिसी लागू करण्यासाठी प्रारंभिक कनेक्शनवर Captive Portal वापरले जाऊ शकते. जेव्हा लोकॅमचे तात्पुरते AD अकाउंट त्यांच्या एंगेजमेंटच्या शेवटी डिसेबल केले जाते, तेव्हा त्यांचा वायरलेस ॲक्सेस आपोआप रद्द होतो.
सराव प्रश्न
Q1. हॉस्पिटलमध्ये एक नवीन विंग जोडली जात आहे, आणि फॅसिलिटीज टीमला औषध साठवणुकीच्या फ्रिजमध्ये वायरलेस तापमान सेन्सर्स तैनात करायचे आहेत. हे सेन्सर्स फक्त WPA2-Personal (Pre-Shared Key) ला सपोर्ट करतात आणि 802.1X वापरू शकत नाहीत. नेटवर्क आर्किटेक्टने यांना सुरक्षितपणे कसे इंटिग्रेट करावे?
टीप: किमान विशेषाधिकाराच्या तत्त्वाचा विचार करा आणि नॉन-कंप्लायंट उपकरणांना क्लिनिकल सिस्टीम्सपासून कसे वेगळे करावे याचा विचार करा.
नमुना उत्तर पहा
आर्किटेक्टने विशिष्ट 'Facilities IoT' VLAN शी मॅप केलेला एक समर्पित, लपलेला SSID तयार केला पाहिजे. सेन्सर्स PSK वापरून कनेक्ट होतील. महत्त्वाचे म्हणजे, या VLAN वर कठोर फायरवॉल ACLs लागू केले जाणे आवश्यक आहे, जे सेन्सर्सना केवळ त्यांच्या विशिष्ट सेंट्रल मॅनेजमेंट सर्व्हरशी संवाद साधण्याची परवानगी देतात आणि इतर सर्व ट्रॅफिक नाकारतात — विशेषतः क्लिनिकल VLAN किंवा इंटरनेटवरील राउटिंग. MAC ऑथेंटिकेशन बायपास (MAB) देखील कॉन्फिगर केले जावे जेणेकरून केवळ खरेदी केलेल्या सेन्सर्सच्या विशिष्ट MAC ॲड्रेसेसना त्या VLAN वर परवानगी मिळेल, ज्यामुळे रोग (rogue) उपकरणांना तोच PSK वापरून जॉईन होण्यापासून प्रतिबंधित करता येईल.
Q2. सकाळच्या व्यस्त शिफ्ट दरम्यान, नर्सेस तक्रार करतात की वॉर्डच्या एका टोकाकडून दुसऱ्या टोकाकडे चालत असताना त्यांच्या टॅब्लेट्सचे EHR सिस्टीमशी असलेले कनेक्शन वारंवार ड्रॉप होत आहे, ज्यामुळे त्यांना पुन्हा लॉग इन करावे लागत आहे. वायरलेस कव्हरेज सर्वेक्षण संपूर्ण वॉर्डमध्ये मजबूत सिग्नल स्ट्रेंथ दर्शवते. याचे संभाव्य कारण आणि उपाय काय आहे?
टीप: मजबूत सिग्नल ॲक्सेस पॉइंट्स दरम्यान अखंड ट्रान्झिशन्सची हमी देत नाही. प्रत्येक AP ट्रान्झिशनवरील ऑथेंटिकेशन ओव्हरहेडचा विचार करा.
नमुना उत्तर पहा
याचे संभाव्य कारण फास्ट रोमिंग प्रोटोकॉल्सचा अभाव आहे. टॅब्लेट एका AP च्या कव्हरेजमधून बाहेर पडून दुसऱ्याशी कनेक्ट होत असताना, त्याला RADIUS सर्व्हरच्या विरूद्ध पूर्ण 802.1X री-ऑथेंटिकेशन करण्यास भाग पाडले जात आहे, ज्यामुळे EHR ॲप्लिकेशन सेशन टाइम आउट होण्याइतकी लेटन्सी निर्माण होते. यावरील उपाय म्हणजे वायरलेस कंट्रोलर्सवर 802.11r (Fast BSS Transition) सक्षम करणे, जे क्लायंटला पूर्ण री-ऑथेंटिकेशन सायकलच्या लेटन्सीशिवाय APs दरम्यान सुरक्षितपणे रोम करण्याची परवानगी देते. ट्रान्झिशन होण्यापूर्वी उपकरणाला इष्टतम टार्गेट AP ओळखण्यात मदत करण्यासाठी 802.11k देखील सक्षम केले जावे.
Q3. एक NHS ट्रस्ट त्याच्या वार्षिक DSP टूलकिट मूल्यांकनाची तयारी करत आहे. ऑडिटरच्या लक्षात येते की प्रशासकीय कर्मचारी स्टाफ WiFi नेटवर्कमध्ये प्रवेश करण्यासाठी शेअर्ड पासवर्ड वापरतात. येथे ओळखलेला प्राथमिक धोका कोणता आहे आणि शिफारस केलेला उपाय काय आहे?
टीप: वैयक्तिक जबाबदारी आणि कर्मचारी संस्था सोडतात तेव्हा ॲक्सेस लाइफसायकलवर लक्ष केंद्रित करा.
नमुना उत्तर पहा
प्राथमिक धोका हा वैयक्तिक जबाबदारीचा अभाव आणि खराब ॲक्सेस लाइफसायकल मॅनेजमेंट हा आहे. जर एखादा प्रशासकीय कर्मचारी ट्रस्ट सोडून गेला, तर शेअर्ड पासवर्ड वैध राहतो, ज्यामुळे संभाव्यतः अनधिकृत प्रवेश मिळू शकतो. शिवाय, नेटवर्कवर कोणत्या विशिष्ट वापरकर्त्याने कोणती कृती केली याचे ऑडिट करणे अशक्य आहे. यावरील उपाय म्हणजे शेअर्ड पासवर्ड (PSK) नेटवर्क बंद करणे आणि प्रशासकीय कर्मचाऱ्यांना त्यांच्या ॲक्टिव्ह डिरेक्टरी क्रेडेंशियल्ससह PEAP-MSCHAPv2 वापरून 802.1X ऑथेंटिकेटेड नेटवर्कवर मायग्रेट करणे. हे वैयक्तिक जबाबदारी सुनिश्चित करते आणि जेव्हा त्यांचे AD अकाउंट नोकरी सोडल्यावर डिसेबल केले जाते तेव्हा आपोआप ॲक्सेस रद्द होतो, जे ॲक्सेस कंट्रोल आणि ऑडिट लॉगिंगसाठी DSP टूलकिटच्या आवश्यकता थेट पूर्ण करते.
या मालिकेमध्ये पुढे वाचा
Cisco SUDI समजून घेणे: Secure Network Access Control मधील Hardware-Anchored Identity
हे मार्गदर्शक स्पष्ट करते की Cisco SUDI कशा प्रकारे एंटरप्राइझ नेटवर्क इन्फ्रास्ट्रक्चरसाठी hardware-anchored, गुपित-सुरक्षित (cryptographically secure) ओळख प्रदान करते. तुमच्या वेन्यूच्या नेटवर्क ॲक्सेस कंट्रोल सुरक्षित करण्यासाठी स्पूफ करता येण्याजोग्या MAC ॲड्रेसेस ऐवजी अपरिवर्तनीय 802.1AR सर्टिफिकेट्स वापरण्याची पद्धत जाणून घ्या.
स्वयंचलित Enterprise WiFi प्रमाणपत्र नावनोंदणीसाठी SCEP कसे कॉन्फिगर करावे
हे मार्गदर्शक स्वयंचलित Enterprise WiFi प्रमाणपत्र नावनोंदणीसाठी SCEP (Simple Certificate Enrollment Protocol) कसे कॉन्फिगर करावे हे स्पष्ट करते, ज्यामध्ये PKI आणि NDES पासून ते MDM प्रोफाइल अंमलबजावणी आणि RADIUS प्रमाणीकरणापर्यंतच्या संपूर्ण आर्किटेक्चरचा समावेश आहे. हे हॉटेल्स, रिटेल साखळी, स्टेडियम, कॉन्फरन्स सेंटर्स आणि सार्वजनिक क्षेत्रातील संस्थांमधील IT व्यवस्थापक, नेटवर्क आर्किटेक्ट्स आणि CTOs ना उद्देशून आहे ज्यांना प्री-शेअर्ड की च्या पलीकडे जाऊन स्केलेबल, ओळख-आधारित 802.1X EAP-TLS प्रमाणीकरण लागू करायचे आहे. Purple चे हार्डवेअर-स्वतंत्र, क्लाउड ओव्हरले प्लॅटफॉर्म थेट या आर्किटेक्चरसह समाकलित होते, जे तुमच्या प्रमाणपत्र-प्रमाणित कर्मचारी नेटवर्कसह अतिथी आणि BYOD WiFi स्तर प्रदान करते.
स्वयंचलित WiFi प्रमाणपत्र नोंदणीसाठी SCEP कसे लागू करावे
हे मार्गदर्शक एंटरप्राइझ ठिकाणी स्वयंचलित WiFi प्रमाणपत्र नोंदणीसाठी SCEP (Simple Certificate Enrollment Protocol) कसे लागू करावे हे स्पष्ट करते. यामध्ये PKI डिझाइन आणि MDM एकत्रीकरणापासून ते अनिवार्य तीन-चरण उपयोजन क्रमापर्यंतच्या संपूर्ण आर्किटेक्चरल ब्ल्यूप्रिंटचा समावेश आहे - आणि IT व्यवस्थापक व नेटवर्क आर्किटेक्ट्सना शेअर केलेले क्रेडेंशियल्स कसे काढून टाकावे, प्रमाणपत्र जीवनचक्र व्यवस्थापन स्वयंचलित कसे करावे आणि मोठ्या प्रमाणावर PCI-DSS व GDPR आवश्यकता कशा पूर्ण कराव्यात हे दाखवते.