NHS Staff WiFi: Come distribuire reti wireless sicure nel settore sanitario
Questa guida di riferimento tecnico descrive in dettaglio l'architettura, i protocolli di sicurezza e le strategie di distribuzione per il NHS Staff WiFi, coprendo l'autenticazione 802.1X, la segmentazione VLAN, le policy BYOD e la conformità al DSP Toolkit. Fornisce indicazioni pratiche per i leader IT sulla distribuzione di reti wireless di livello enterprise che servono utenti clinici, amministrativi e ospiti su un'infrastruttura fisica condivisa senza compromettere la sicurezza. Sia che stiate pianificando una nuova installazione o mettendo in sicurezza un parco dispositivi esistente, questa guida fornisce i framework decisionali e i passaggi di implementazione necessari per agire in questo trimestre.
Ascolta questa guida
Visualizza trascrizione del podcast
📚 Parte della nostra serie principale: Enterprise WiFi Security Guide →

कार्यकारी सारांश
NHS संपत्तियों में सुरक्षित, विश्वसनीय WiFi तैनात करना अब कोई वैकल्पिक सुविधा नहीं है — यह एक महत्वपूर्ण नैदानिक बुनियादी ढांचा (clinical infrastructure) है। मोबाइल-फर्स्ट रोगी देखभाल, इलेक्ट्रॉनिक स्वास्थ्य रिकॉर्ड (EHR), और जुड़े हुए चिकित्सा उपकरणों की ओर बढ़ता झुकाव एक ऐसे वायरलेस आर्किटेक्चर की मांग करता है जो कड़े सुरक्षा नियंत्रणों के साथ निर्बाध रोमिंग को संतुलित करे।
IT प्रबंधकों, नेटवर्क आर्किटेक्ट्स और CTOs के लिए, मुख्य चुनौती सुरक्षा से समझौता किए बिना साझा भौतिक बुनियादी ढांचे पर विभिन्न उपयोगकर्ता समूहों — नैदानिक कर्मचारियों, प्रशासनिक कर्मियों, रोगियों और मेहमानों — को समायोजित करना है, जो NHS डेटा सुरक्षा और संरक्षण (DSP) टूलकिट आवश्यकताओं को पूरा करता हो। यह मार्गदर्शिका NHS स्टाफ WiFi के लिए तकनीकी आवश्यकताओं का विवरण देती है, जिसमें IEEE 802.1X जैसे मजबूत प्रमाणीकरण ढांचे, VLANs के माध्यम से तार्किक नेटवर्क विभाजन (logical network segmentation), और Bring Your Own Device (BYOD) एंडपॉइंट्स के सुरक्षित ऑनबोर्डिंग पर ध्यान केंद्रित किया गया है।
विरासत (legacy) प्री-शेयर्ड कीज़ (PSK) से दूर जाकर और पहचान-संचालित एक्सेस नीतियों को अपनाकर, स्वास्थ्य सेवा संगठन उल्लंघन के जोखिम को कम कर सकते हैं, परिचालन संबंधी बाधाओं को कम कर सकते हैं, और डिजिटल परिवर्तन कार्यक्रमों के लिए वायरलेस आधार प्रदान कर सकते हैं। इसका व्यावसायिक पक्ष भी उतना ही मजबूत है: हेल्पडेस्क ओवरहेड में कमी, प्रमाणित DSP टूलकिट अनुपालन, और एक ऐसा नेटवर्क जो बिना किसी पूर्ण बुनियादी ढांचे के पुनर्निर्माण के भविष्य के नैदानिक नवाचारों का समर्थन करने में सक्षम हो।
तकनीकी गहन विश्लेषण
प्रमाणीकरण और एक्सेस नियंत्रण
एक सुरक्षित स्वास्थ्य सेवा वायरलेस नेटवर्क की नींव पहचान-आधारित एक्सेस नियंत्रण है। प्री-शेयर्ड कीज़ का उपयोग करने वाले विरासत WPA2-Personal नेटवर्क नैदानिक वातावरण के लिए मौलिक रूप से अनुपयुक्त हैं। वे कोई व्यक्तिगत जवाबदेही प्रदान नहीं करते हैं, कर्मचारियों के जाने पर ऑनबोर्डिंग हटाने की प्रक्रिया को जटिल बनाते हैं, और क्रेडेंशियल के साथ समझौता होने या इच्छित समूह से बाहर साझा किए जाने पर विफलता का एक एकल बिंदु (single point of failure) पेश करते हैं।
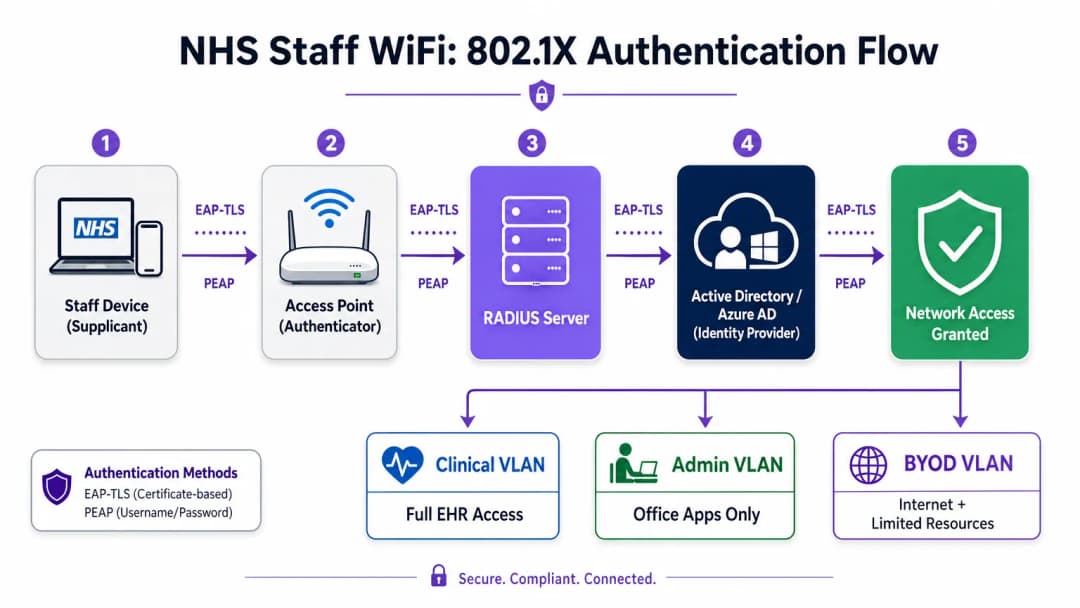
आधुनिक NHS तैनाती में WPA3-Enterprise (या न्यूनतम संक्रमण स्थिति के रूप में WPA2-Enterprise) को IEEE 802.1X प्रमाणीकरण का उपयोग करके अनिवार्य किया जाना चाहिए। इस ढांचे के लिए आवश्यक है कि नेटवर्क एक्सेस दिए जाने से पहले प्रत्येक उपयोगकर्ता या डिवाइस अद्वितीय क्रेडेंशियल प्रस्तुत करे, और उस प्रमाणीकरण का परिणाम यह निर्धारित करता है कि डिवाइस को किस तार्किक नेटवर्क सेगमेंट पर रखा जाए।
स्वास्थ्य सेवा तैनाती में दो EAP तरीके हावी हैं:
| EAP तरीका | प्रमाणीकरण तंत्र | इसके लिए सबसे उपयुक्त | सुरक्षा स्तर |
|---|---|---|---|
| EAP-TLS | क्लाइंट-साइड डिजिटल प्रमाणपत्र | कॉर्पोरेट-प्रबंधित नैदानिक उपकरण | उच्चतम — फ़िशिंग के लिए कोई पासवर्ड नहीं |
| PEAP-MSCHAPv2 | एन्क्रिप्टेड टनल में उपयोगकर्ता नाम/पासवर्ड | BYOD, व्यवस्थापक कर्मचारी, विरासत उपकरण | उच्च — TLS द्वारा सुरक्षित क्रेडेंशियल |
EAP-TLS कॉर्पोरेट उपकरणों के लिए स्वर्ण मानक (gold standard) है। प्रमाणपत्रों को मोबाइल डिवाइस मैनेजमेंट (MDM) प्लेटफॉर्म के माध्यम से वितरित किया जाता है, जिससे ज़ीरो-टच प्रमाणीकरण सक्षम होता है — डिवाइस पृष्ठभूमि में चुपचाप प्रमाणित हो जाता है। PEAP-MSCHAPv2 एक एन्क्रिप्टेड TLS सत्र के भीतर एक्टिव डायरेक्ट्री या एज़्योर AD क्रेडेंशियल को सुरक्षित रूप से टनल करता है, जिससे यह BYOD परिदृश्यों के लिए उपयुक्त हो जाता है जहां प्रमाणपत्र प्रबंधन व्यावहारिक नहीं है।
वायरलेस बुनियादी ढांचे को संगठन के केंद्रीय पहचान प्रदाता (IdP) के साथ एकीकृत करना यह सुनिश्चित करता है कि किसी कर्मचारी का AD खाता अक्षम होने पर एक्सेस स्वचालित रूप से रद्द हो जाए, जो सीधे एक्सेस लाइफसाइकल प्रबंधन के लिए DSP टूलकिट आवश्यकताओं को पूरा करता है।
नेटवर्क विभाजन और ट्रस्ट ज़ोन
भौतिक एक्सेस पॉइंट पूरे अस्पताल के फर्श पर प्रसारण करते हैं, लेकिन तार्किक विभाजन यह सुनिश्चित करता है कि न्यूनतम विशेषाधिकार के सिद्धांत के आधार पर ट्रैफ़िक अलग रहे। स्वास्थ्य सेवा सेटिंग में एक फ्लैट नेटवर्क आर्किटेक्चर एक गंभीर सुरक्षा भेद्यता है, जो एक समझौता किए गए अतिथि डिवाइस या कमजोर IoT सेंसर को संभावित रूप से नैदानिक प्रणालियों तक पहुँचने की अनुमति देता है।
सर्वोत्तम अभ्यास विशिष्ट SSIDs के लिए मैप किए गए अलग वर्चुअल लोकल एरिया नेटवर्क (VLANs) बनाने का निर्देश देता है, जिसमें फ़ायरवॉल नियम उनके बीच ट्रैफ़िक सीमाओं को लागू करते हैं:
| ज़ोन | SSID | प्रमाणीकरण | एक्सेस | QoS प्राथमिकता |
|---|---|---|---|---|
| नैदानिक | NHS-Clinical | EAP-TLS (प्रमाणपत्र) | EHR, PACS, नैदानिक संदेश सेवा | उच्चतम |
| प्रशासनिक | NHS-Staff | PEAP (AD क्रेडेंशियल) | ऑफिस ऐप्स, इंटरनेट | मध्यम |
| मेडिकल IoT | Hidden/MAB | MAC Authentication Bypass | केवल डिवाइस कंट्रोलर | उच्च |
| अतिथि / रोगी | NHS-Guest | Captive Portal | केवल इंटरनेट | निम्न |
| BYOD | NHS-BYOD | PEAP (AD क्रेडेंशियल) | इंटरनेट, सीमित VDI | निम्न |
मेडिकल IoT VLAN विशेष ध्यान देने योग्य है। कई जुड़े हुए चिकित्सा उपकरण — इन्फ्यूजन पंप, रोगी मॉनिटर, वायरलेस कॉल सिस्टम — 802.1X का समर्थन नहीं कर सकते हैं। MAC Authentication Bypass (MAB) इसका विकल्प है, लेकिन इसे सख्त फ़ायरवॉल एक्सेस कंट्रोल लिस्ट (ACLs) के साथ जोड़ा जाना चाहिए जो इन उपकरणों को केवल उनके निर्दिष्ट प्रबंधन सर्वर के साथ संचार करने तक सीमित करते हैं।
BYOD की चुनौती
Bring Your Own Device नीतियां प्रशासनिक कर्मचारियों और आने वाले चिकित्सकों के लिए तेजी से आम हो रही हैं। हालांकि, अप्रबंधित व्यक्तिगत उपकरण एक महत्वपूर्ण जोखिम का प्रतिनिधित्व करते हैं यदि उन्हें विश्वसनीय नेटवर्क सेगमेंट पर जाने की अनुमति दी जाती है।
एक सुरक्षित BYOD तैनाती में इन उपकरणों को एक समर्पित BYOD VLAN पर ऑनबोर्ड करना शामिल है। यह ज़ोन इंटरनेट एक्सेस प्रदान करता है और शायद एक सुरक्षित गेटवे या वर्चुअल डेस्कटॉप इंफ्रास्ट्रक्चर (VDI) के माध्यम से विशिष्ट, गैर-संवेदनशील आंतरिक संसाधनों तक सीमित पहुंच प्रदान करता है। इसमें नैदानिक प्रणालियों या रोगी डेटा स्टोर के लिए सीधे रूटिंग की अनुमति बिल्कुल नहीं होनी चाहिए।

कार्यान्वयन मार्गदर्शिका
एक सुरक्षित NHS स्टाफ WiFi आर्किटेक्चर को तैनात करने के लिए चल रहे नैदानिक संचालन में व्यवधान को कम करने के लिए चरणबद्ध दृष्टिकोण की आवश्यकता होती है।
चरण 1: मूल्यांकन और डिज़ाइन
एक व्यापक वायरलेस साइट सर्वेक्षण के साथ शुरुआत करें। लीड-लाइनेड दीवारों, भारी मशीनरी और घनी आबादी के कारण स्वास्थ्य सेवा वातावरण रेडियो फ्रीक्वेंसी (RF) प्रसार के लिए कुख्यात रूप से कठिन हैं। डिज़ाइन में केवल कवरेज ही नहीं, बल्कि क्षमता का भी ध्यान रखा जाना चाहिए, जिससे आपातकालीन विभागों और बाह्य रोगी क्लीनिकों जैसे उच्च-यातायात वाले क्षेत्रों में पर्याप्त एक्सेस पॉइंट घनत्व सुनिश्चित हो सके।
आवश्यक SSIDs को परिभाषित करें और उन्हें संबंधित VLANs और सुरक्षा नीतियों से मैप करें। प्रसारण SSIDs की संख्या को न्यूनतम रखें — आदर्श रूप से चार से अधिक नहीं — ताकि प्रबंधन ओवरहेड को कम किया जा सके और बीकन फ्रेम कंजेशन को कम किया जा सके, जो समग्र नेटवर्क प्रदर्शन को कम करता है।
चरण 2: बुनियादी ढांचा कॉन्फ़िगरेशन
परिभाषित VLANs का समर्थन करने के लिए कोर स्विचिंग और रूटिंग बुनियादी ढांचे को कॉन्फ़िगर करें। न्यूनतम विशेषाधिकार लागू करने के लिए सेगमेंट के बीच की सीमाओं पर फ़ायरवॉल नियम लागू करें। RADIUS सर्वर (जैसे, Cisco ISE, Aruba ClearPass, या क्लाउड-आधारित RADIUS-as-a-Service) सेट करें और इसे केंद्रीय पहचान प्रदाता के साथ एकीकृत करें। जिन वातावरणों में Purple का प्लेटफ़ॉर्म तैनात है, वहां इस चरण में WiFi Analytics को एकीकृत करना नेटवर्क उपयोग, रोमिंग पैटर्न और क्षमता हॉटस्पॉट में दृश्यता प्रदान करता है।
चरण 3: नीति प्रवर्तन और ऑनबोर्डिंग
प्रमाणीकरण नीतियां तैनात करें। कॉर्पोरेट उपकरणों के लिए, आवश्यक वायरलेस प्रोफाइल और क्लाइंट प्रमाणपत्र (EAP-TLS के लिए) भेजने के लिए MDM समाधान का उपयोग करें। यह सुनिश्चित करता है कि प्रबंधित उपकरण उपयोगकर्ता के हस्तक्षेप के बिना स्वचालित रूप से और सुरक्षित रूप से कनेक्ट हों।
BYOD के लिए, एक स्पष्ट ऑनबोर्डिंग वर्कफ़्लो स्थापित करें — आमतौर पर एक ऑनबोर्डिंग पोर्टल जो उपयोगकर्ता को उनके कॉर्पोरेट क्रेडेंशियल के साथ प्रमाणित करने, स्वीकार्य उपयोग नीति को स्वीकार करने और डिवाइस को सुरक्षित BYOD VLAN पर ले जाने के माध्यम से मार्गदर्शन करता है। Purple के Guest WiFi प्लेटफ़ॉर्म को रोगी और अतिथि SSID के लिए Captive Portal परत के रूप में तैनात किया जा सकता है, जो बड़े पैमाने पर GDPR-अनुरूप डेटा कैप्चर और शर्तों की स्वीकृति को संभालता है।
चरण 4: परीक्षण और सत्यापन
गो-लाइव से पहले, प्रत्येक प्रमाणीकरण पथ, VLAN असाइनमेंट और फ़ायरवॉल नियम का एंड-टू-एंड परीक्षण करें। विशेष रूप से पुनः प्रमाणीकरण घटनाओं की निगरानी करते हुए एक परीक्षण डिवाइस के साथ नैदानिक फर्श पर चलकर रोमिंग व्यवहार को मान्य करें। पुष्टि करें कि फास्ट रोमिंग प्रोटोकॉल (802.11r और 802.11k) सही ढंग से काम कर रहे हैं और एप्लिकेशन सत्र AP संक्रमणों के बाद भी बने रहते हैं।
सर्वोत्तम अभ्यास
प्री-शेयर्ड कीज़ को समाप्त करें। व्यक्तिगत जवाबदेही और केंद्रीकृत एक्सेस नियंत्रण सुनिश्चित करने के लिए सभी कर्मचारियों और नैदानिक नेटवर्क को 802.1X प्रमाणीकरण पर स्थानांतरित करें। यह DSP टूलकिट अनुपालन के लिए एक गैर-परक्राम्य आवश्यकता है।
सख्त विभाजन लागू करें। अतिथि, BYOD, या IoT ट्रैफ़िक को कभी भी नैदानिक डेटा के समान तार्किक सेगमेंट पर अनुमति न दें। डिफ़ॉल्ट नीति के रूप में स्पष्ट अस्वीकार (deny) नियमों के साथ, इंटर-VLAN रूटिंग को नियंत्रित करने के लिए स्टेटफुल फ़ायरवॉल का उपयोग करें।
नैदानिक ट्रैफ़िक को प्राथमिकता दें। विशेष रूप से उच्च भीड़ की अवधि के दौरान, अतिथि या प्रशासनिक ट्रैफ़िक की तुलना में नैदानिक अनुप्रयोगों — वॉयस ओवर WLAN, EHR एक्सेस — को प्राथमिकता देने के लिए वायरलेस कंट्रोलर और स्विच पर QoS नीतियां लागू करें।
फास्ट रोमिंग सक्षम करें। 802.11r (फास्ट BSS ट्रांज़िशन) और 802.11k (रेडियो रिसोर्स मेजरमेंट) को तैनात करें ताकि यह सुनिश्चित हो सके कि नैदानिक कर्मचारी एप्लिकेशन टाइमआउट या टूटे हुए कनेक्शन का अनुभव किए बिना सुविधा के माध्यम से आगे बढ़ सकें।
निरंतर निगरानी। नेटवर्क स्वास्थ्य की निगरानी करने, अनधिकृत एक्सेस पॉइंट की पहचान करने और उपयोगकर्ता रोमिंग व्यवहार को ट्रैक करने के लिए एनालिटिक्स प्लेटफॉर्म का उपयोग करें। फुटफॉल और उपयोग के पैटर्न को समझना — Retail और Hospitality वातावरण में सिद्ध एक तकनीक — क्षमता योजना और समस्या निवारण के लिए अस्पताल की सेटिंग में भी उतनी ही मूल्यवान है।
नियमित ऑडिटिंग। जहां लागू हो, DSP टूलकिट, साइबर एसेंशियल प्लस और ISO 27001 के साथ निरंतर अनुपालन सुनिश्चित करने के लिए वार्षिक वायरलेस जोखिम मूल्यांकन आयोजित करें।
समस्या निवारण और जोखिम शमन
प्रमाणीकरण टाइमआउट
उच्च क्लाइंट घनत्व वाले वातावरण में, RADIUS सर्वर अभिभूत हो सकते हैं, जिससे प्रमाणीकरण टाइमआउट और टूटे हुए कनेक्शन हो सकते हैं। सुनिश्चित करें कि RADIUS बुनियादी ढांचा पर्याप्त रूप से स्केल किया गया है और अत्यधिक उपलब्ध है। कई प्रमाणीकरण सर्वरों में लोड बैलेंसिंग लागू करें और एक प्रमुख परिचालन मीट्रिक के रूप में RADIUS प्रतिक्रिया समय की निगरानी करें।
रोमिंग के मुद्दे
वार्डों के बीच तेजी से चलने वाले नैदानिक कर्मचारियों को टूटे हुए कनेक्शन का अनुभव हो सकता है यदि वायरलेस बुनियादी ढांचा फास्ट रोमिंग प्रोटोकॉल का समर्थन नहीं करता है। वायरलेस कंट्रोलर पर 802.11r और 802.11k सक्षम करें और सुनिश्चित करें कि क्लाइंट डिवाइस इन मानकों का समर्थन करते हैं। कवरेज अंतराल या 'स्टिकी क्लाइंट' मुद्दों की पहचान करने और उन्हें हल करने के लिए पोस्ट-डिप्लॉयमेंट रोमिंग सर्वेक्षण आयोजित करें, जहां एक डिवाइस करीब जाने के बजाय दूर के, कमजोर AP से चिपका रहता है।
विरासत डिवाइस असंगतता
पुराने चिकित्सा उपकरण WPA3 या 802.1X जैसे आधुनिक सुरक्षा प्रोटोकॉल का समर्थन नहीं कर सकते हैं। MAB का उपयोग करके इन उपकरणों को एक समर्पित IoT VLAN पर अलग करें। उनके संचार को केवल आवश्यक प्रबंधन सर्वर तक सीमित करने के लिए सख्त फ़ायरवॉल नियम लागू करें। उन महत्वपूर्ण उपकरणों के लिए हार्डवेयर अपग्रेड या वायरलेस ब्रिज पर विचार करें जिन्हें मूल रूप से सुरक्षित नहीं किया जा सकता है।
प्रमाणपत्र की समाप्ति
EAP-TLS तैनाती परिभाषित समाप्ति अवधि वाले प्रमाणपत्रों पर निर्भर करती है। यदि प्रमाणपत्र नवीनीकरण के बिना समाप्त हो जाते हैं, तो डिवाइस प्रमाणित करने में विफल हो जाएंगे, जिससे व्यापक नैदानिक व्यवधान होगा। MDM प्लेटफॉर्म के माध्यम से SCEP (सिंपल सर्टिफिकेट एनरोलमेंट प्रोटोकॉल) के माध्यम से स्वचालित प्रमाणपत्र नवीनीकरण लागू करें, और सक्रिय रूप से प्रमाणपत्र समाप्ति तिथियों की निगरानी करें।
ROI और व्यावसायिक प्रभाव
एक सुरक्षित, एंटरप्राइज़-ग्रेड वायरलेस आर्किटेक्चर में निवेश नैदानिक, परिचालन और IT डोमेन में मापने योग्य रिटर्न प्रदान करता है।
नैदानिक दक्षता। विश्वसनीय कनेक्टिविटी यह सुनिश्चित करती है कि चिकित्सकों के पास देखभाल के बिंदु पर रोगी के रिकॉर्ड तक तत्काल पहुंच हो, जिससे जानकारी खोजने या टूटे हुए कनेक्शन से निपटने में लगने वाला समय कम हो जाता है। यह सीधे रोगी थ्रूपुट और देखभाल वितरण की गुणवत्ता को प्रभावित करता है।
कम IT ओवरहेड। साझा पासवर्ड और मैन्युअल ऑनबोर्डिंग से हटकर स्वचालित, प्रमाणपत्र-आधारित प्रमाणीकरण की ओर बढ़ने से पासवर्ड रीसेट और कनेक्टिविटी समस्याओं से संबंधित हेल्पडेस्क टिकटों में काफी कमी आती है। एक NHS ट्रस्ट ने 802.1X पर माइग्रेशन के बाद वायरलेस से संबंधित हेल्पडेस्क कॉल में 40% की कमी दर्ज की।
जोखिम शमन। सख्त विभाजन और मजबूत प्रमाणीकरण DSP टूलकिट आवश्यकताओं को पूरा करने, डेटा उल्लंघनों या अनुपालन विफलताओं से जुड़े वित्तीय और प्रतिष्ठित जोखिमों को कम करने के लिए मौलिक हैं। डेटा उल्लंघन की लागत उचित रूप से तैयार की गई वायरलेस संपत्ति में निवेश से कहीं अधिक है।
भविष्य के लिए तैयार करना (Future-Proofing)। एक अच्छी तरह से डिज़ाइन किया गया वायरलेस नेटवर्क भविष्य की डिजिटल स्वास्थ्य पहलों — स्थान-आधारित सेवाएं, रीयल-टाइम एसेट ट्रैकिंग, उन्नत टेलीहेल्थ एप्लिकेशन — के लिए आधार प्रदान करता है, जो Healthcare और Transport जैसे संबंधित क्षेत्रों में व्यापक रणनीतिक लक्ष्यों के साथ संरेखित होता है जहां मोबाइल कनेक्टिविटी परिचालन दक्षता को रेखांकित करती है।
उन संगठनों के लिए जो यह समझना चाहते हैं कि Purple का प्लेटफ़ॉर्म इस आर्किटेक्चर के अतिथि और रोगी WiFi परत से कैसे मेल खाता है, Healthcare उद्योग पृष्ठ NHS-संगत Captive Portal, एनालिटिक्स और GDPR-अनुरूप डेटा हैंडलिंग क्षमताओं का एक विस्तृत अवलोकन प्रदान करता है। वही एनालिटिक्स सिद्धांत जो Retail में ग्राहक जुड़ाव को बढ़ावा देते हैं, सीधे अस्पताल संपदा टीमों के लिए परिचालन खुफिया में अनुवादित होते हैं।
Definizioni chiave
IEEE 802.1X
Uno standard IEEE per il controllo dell'accesso alla rete basato su porta (PNAC). Fornisce un meccanismo di autenticazione per i dispositivi che desiderano connettersi a una LAN o WLAN, richiedendo a ciascun dispositivo di presentare le credenziali prima di ottenere l'accesso.
Questo è lo standard obbligatorio per sostituire le password condivise non sicure con accessi individuali basati sull'identità per il personale e i dispositivi clinici. È la pietra angolare di un'architettura wireless conforme al DSP Toolkit.
VLAN (Virtual Local Area Network)
Una sottorete logica che raggruppa una serie di dispositivi provenienti da diversi segmenti di rete fisica. Le VLAN consentono agli amministratori di rete di partizionare una singola rete commutata per soddisfare i requisiti funzionali e di sicurezza di diversi gruppi di utenti.
Le VLAN sono essenziali per segmentare il traffico clinico da quello degli ospiti e amministrativo, limitando il raggio d'azione di una potenziale violazione della sicurezza e applicando il principio del privilegio minimo.
RADIUS (Remote Authentication Dial-In User Service)
Un protocollo di rete che fornisce una gestione centralizzata di autenticazione, autorizzazione e contabilità (AAA) per gli utenti che si connettono e utilizzano un servizio di rete.
Il server RADIUS funge da motore decisionale tra gli access point wireless e il database centrale delle identità (Active Directory), decidendo chi ottiene l'accesso e a quale VLAN viene assegnato.
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
Un metodo EAP che si affida a certificati client e server per stabilire una connessione sicura e reciprocamente autenticata. Nessuna delle due parti si fida dell'altra senza un certificato valido.
Il metodo più sicuro per autenticare i dispositivi di proprietà dell'ospedale. I certificati distribuiti tramite MDM garantiscono che solo gli endpoint gestiti e attendibili possano accedere alla rete clinica, senza password soggette a phishing o condivisione.
MAB (MAC Authentication Bypass)
Un metodo di autenticazione dei dispositivi basato sul loro indirizzo MAC hardware, utilizzato come alternativa per i dispositivi che non supportano l'802.1X.
Necessario per i dispositivi IoT medici legacy che necessitano di accesso alla rete ma non sono in grado di gestire protocolli di autenticazione complessi. Deve essere sempre associato a rigide ACL del firewall per limitare il dispositivo ai percorsi di comunicazione consentiti.
DSP Toolkit (Data Security and Protection Toolkit)
Uno strumento di autovalutazione online richiesto da NHS England che tutte le organizzazioni devono completare se hanno accesso ai dati e ai sistemi dei pazienti del NHS. Si mappa sui dieci standard di sicurezza dei dati del National Data Guardian.
La conformità al DSP Toolkit è obbligatoria per le organizzazioni del NHS e i loro fornitori. Una solida sicurezza wireless — inclusi 802.1X, segmentazione e gestione del ciclo di vita degli accessi — è un componente critico per dimostrare la conformità.
SSID (Service Set Identifier)
Il nome primario associato a una rete locale wireless 802.11, trasmesso dagli access point per consentire ai dispositivi client di identificare e connettersi alla rete.
Gli ospedali dovrebbero ridurre al minimo il numero di SSID trasmessi (ad es. NHS-Clinical, NHS-Guest) per ridurre il sovraccarico di gestione e di radiofrequenza. Ogni SSID dovrebbe essere mappato su una policy di sicurezza e una VLAN specifiche.
QoS (Quality of Service)
Tecnologie che gestiscono il traffico dati per ridurre la perdita di pacchetti, la latenza e il jitter su una rete, dando priorità ad alcuni tipi di traffico rispetto ad altri.
Cruciale nel settore sanitario per garantire che le applicazioni cliniche critiche per la vita e le comunicazioni vocali abbiano sempre la priorità rispetto a traffico meno importante, come lo streaming video degli ospiti o gli aggiornamenti software.
802.11r (Fast BSS Transition)
Un emendamento IEEE che consente il roaming rapido tra gli access point pre-autenticando il client sull'AP di destinazione prima che avvenga la transizione fisica, riducendo drasticamente la latenza di roaming.
Essenziale per gli ambienti clinici in cui il personale è costantemente in movimento. Senza 802.11r, i dispositivi devono eseguire una riautenticazione RADIUS completa a ogni passaggio di AP, il che può causare il timeout delle sessioni applicative.
Esempi pratici
Un Trust del NHS sta distribuendo nuove postazioni di lavoro mobili (Workstations on Wheels) in diversi reparti. Il team IT deve garantire che questi dispositivi mantengano la connettività mentre gli infermieri si spostano tra i vari access point, garantendo al contempo che solo i dispositivi autorizzati possano accedere alla VLAN clinica contenente il sistema della cartella clinica elettronica.
Il Trust dovrebbe implementare un framework di autenticazione 802.1X utilizzando EAP-TLS. Il team IT utilizzerà la propria soluzione MDM per inviare un certificato client univoco e il profilo wireless corrispondente a ciascuna postazione di lavoro. I controller wireless saranno configurati per autenticare questi dispositivi tramite un server RADIUS, che verifica il certificato rispetto alla PKI interna. Una volta completata con successo l'autenticazione, il server RADIUS assegna dinamicamente la postazione di lavoro alla VLAN clinica dedicata tramite un attributo RADIUS (ad es. Tunnel-Private-Group-ID). Per soddisfare i requisiti di roaming, i protocolli 802.11r (Fast BSS Transition) e 802.11k (Radio Resource Measurement) devono essere abilitati sull'infrastruttura wireless per consentire alle postazioni di lavoro di passare senza problemi da un access point all'altro senza dover eseguire ogni volta un ciclo completo di riautenticazione sul server RADIUS.
Un ospedale deve fornire l'accesso a Internet ai medici sostituti (locum) in visita che utilizzano i propri laptop personali (BYOD). Questi medici devono accedere a strumenti di riferimento medico basati su cloud, ma deve essere loro rigorosamente vietato l'accesso ai database interni dei pazienti dell'ospedale.
L'ospedale dovrebbe distribuire un SSID BYOD dedicato mappato su una VLAN BYOD isolata. L'autenticazione dovrebbe essere gestita tramite 802.1X utilizzando PEAP-MSCHAPv2, consentendo ai medici sostituti di accedere utilizzando credenziali Active Directory temporanee fornite dalle risorse umane al loro arrivo. Il firewall centrale deve essere configurato con una ACL che neghi esplicitamente qualsiasi instradamento dalla VLAN BYOD alle VLAN cliniche o amministrative, consentendo solo il traffico in uscita verso Internet. Inoltre, è possibile utilizzare un Captive Portal al momento della connessione iniziale per imporre una Acceptable Use Policy prima di concedere l'accesso completo a Internet. Quando l'account AD temporaneo del medico viene disattivato al termine del suo incarico, il suo accesso wireless viene revocato automaticamente.
Domande di esercitazione
Q1. Viene aggiunta una nuova ala all'ospedale e il team delle strutture desidera installare sensori di temperatura wireless nei frigoriferi per la conservazione dei farmaci. Questi sensori supportano solo WPA2-Personal (Pre-Shared Key) e non possono utilizzare l'802.1X. In che modo l'architetto di rete dovrebbe integrarli in modo sicuro?
Suggerimento: Considerate il principio del privilegio minimo e come isolare i dispositivi non conformi dai sistemi clinici.
Visualizza risposta modello
L'architetto dovrebbe creare un SSID dedicato e nascosto mappato su una VLAN specifica 'Facilities IoT'. I sensori si connetteranno utilizzando la PSK. Aspetto fondamentale, a questa VLAN devono essere applicate rigide ACL del firewall, consentendo ai sensori di comunicare solo con il loro server di gestione centrale specifico e negando tutto l'altro traffico — in particolare l'instradamento verso la VLAN clinica o Internet. Dovrebbe essere configurato anche il MAC Authentication Bypass (MAB) per garantire che solo gli indirizzi MAC specifici dei sensori acquistati siano ammessi su quella VLAN, impedendo a dispositivi non autorizzati di connettersi utilizzando la stessa PSK.
Q2. Durante un turno mattutino intenso, gli infermieri segnalano che i loro tablet perdono frequentemente la connessione al sistema EHR mentre percorrono il reparto, richiedendo loro di effettuare nuovamente l'accesso. L'analisi della copertura wireless mostra un'ottima potenza del segnale in tutto il reparto. Qual è la causa probabile e la soluzione?
Suggerimento: Un segnale forte non garantisce transizioni fluide tra gli access point. Considerate il sovraccarico di autenticazione a ogni passaggio di AP.
Visualizza risposta modello
La causa probabile è la mancanza di protocolli di roaming rapido. Quando il tablet si sposta fuori dalla portata di un AP e si connette a quello successivo, è costretto a eseguire una riautenticazione 802.1X completa sul server RADIUS, il che introduce una latenza sufficiente a causare il timeout della sessione dell'applicazione EHR. La soluzione consiste nell'abilitare l'802.11r (Fast BSS Transition) sui controller wireless, consentendo al client di spostarsi in modo sicuro tra gli AP senza la latenza di un ciclo completo di riautenticazione. Dovrebbe essere abilitato anche l'802.11k per aiutare il dispositivo a identificare l'AP di destinazione ottimale prima che avvenga la transizione.
Q3. Un Trust del NHS si sta preparando per la valutazione annuale del DSP Toolkit. L'auditor nota che il personale amministrativo utilizza una password condivisa per accedere alla rete Staff WiFi. Qual è il rischio principale identificato in questo caso e qual è l'intervento correttivo raccomandato?
Suggerimento: Concentratevi sulla responsabilità individuale e sul ciclo di vita degli accessi quando il personale lascia l'organizzazione.
Visualizza risposta modello
Il rischio principale è la mancanza di responsabilità individuale e una scarsa gestione del ciclo di vita degli accessi. Se un membro del personale amministrativo lascia il Trust, la password condivisa rimane valida, consentendo potenzialmente un accesso non autorizzato. Inoltre, è impossibile verificare quale specifico utente abbia eseguito un'azione sulla rete. L'intervento correttivo consiste nel dismettere la rete con password condivisa (PSK) e migrare il personale amministrativo a una rete autenticata 802.1X utilizzando PEAP-MSCHAPv2 con le proprie credenziali Active Directory. Ciò garantisce la responsabilità individuale e la revoca automatica dell'accesso quando il loro account AD viene disattivato al momento della cessazione del rapporto di lavoro, rispondendo direttamente ai requisiti del DSP Toolkit per il controllo degli accessi e la registrazione dei log di controllo.
Continua a leggere questa serie
Comprensione di Cisco SUDI: Identità ancorata all'hardware nel controllo degli accessi di rete sicuro
Questa guida spiega come Cisco SUDI fornisca un'identità crittograficamente sicura e ancorata all'hardware per l'infrastruttura di rete aziendale. Scopri come sostituire gli indirizzi MAC facilmente falsificabili con certificati 802.1AR immutabili per proteggere il controllo degli accessi alla rete della tua struttura.
Come configurare SCEP per la registrazione automatica dei certificati WiFi aziendali
Questa guida spiega come configurare SCEP (Simple Certificate Enrollment Protocol) per la registrazione automatica dei certificati WiFi aziendali, coprendo l'intera architettura, da PKI e NDES fino alla distribuzione dei profili MDM e alla convalida RADIUS. Si rivolge a responsabili IT, architetti di rete e CTO di hotel, catene di vendita al dettaglio, stadi, centri congressi e organizzazioni del settore pubblico che hanno l'esigenza di superare le chiavi precondivise e implementare un'autenticazione 802.1X EAP-TLS scalabile e basata sull'identità. La piattaforma cloud overlay di Purple, indipendente dall'hardware, si integra direttamente con questa architettura, fornendo il livello WiFi per ospiti e BYOD che si affianca alla rete del personale autenticata tramite certificato.
Come implementare SCEP per l'assegnazione automatizzata dei certificati WiFi
Questa guida spiega come implementare SCEP (Simple Certificate Enrollment Protocol) per l'assegnazione automatizzata dei certificati WiFi nelle sedi aziendali. Copre l'intero schema architetturale - dalla progettazione PKI e integrazione MDM alla sequenza obbligatoria di implementazione in tre passaggi - e mostra ai manager IT e agli architetti di rete come eliminare le credenziali condivise, automatizzare la gestione del ciclo di vita dei certificati e soddisfare i requisiti PCI DSS e GDPR su scala globale.