NHS Staff WiFi: How to Deploy Secure Wireless Networks in Healthcare
This technical reference guide details the architecture, security protocols, and deployment strategies for NHS Staff WiFi, covering 802.1X authentication, VLAN segmentation, BYOD policies, and DSP Toolkit compliance. It provides actionable guidance for IT leaders on deploying enterprise-grade wireless networks that serve clinical, administrative, and guest users on shared physical infrastructure without compromising security. Whether you are planning a new deployment or hardening an existing estate, this guide delivers the decision frameworks and implementation steps needed to act this quarter.
Video overview
Listen to this guide
View podcast transcript
📚 Part of our core series: Enterprise WiFi Security Guide →

कार्यकारी सारांश
NHS संपत्तियों में सुरक्षित, विश्वसनीय WiFi तैनात करना अब कोई वैकल्पिक सुविधा नहीं है — यह एक महत्वपूर्ण नैदानिक बुनियादी ढांचा (clinical infrastructure) है। मोबाइल-फर्स्ट रोगी देखभाल, इलेक्ट्रॉनिक स्वास्थ्य रिकॉर्ड (EHR), और जुड़े हुए चिकित्सा उपकरणों की ओर बढ़ता झुकाव एक ऐसे वायरलेस आर्किटेक्चर की मांग करता है जो कड़े सुरक्षा नियंत्रणों के साथ निर्बाध रोमिंग को संतुलित करे।
IT प्रबंधकों, नेटवर्क आर्किटेक्ट्स और CTOs के लिए, मुख्य चुनौती सुरक्षा से समझौता किए बिना साझा भौतिक बुनियादी ढांचे पर विभिन्न उपयोगकर्ता समूहों — नैदानिक कर्मचारियों, प्रशासनिक कर्मियों, रोगियों और मेहमानों — को समायोजित करना है, जो NHS डेटा सुरक्षा और संरक्षण (DSP) टूलकिट आवश्यकताओं को पूरा करता हो। यह मार्गदर्शिका NHS स्टाफ WiFi के लिए तकनीकी आवश्यकताओं का विवरण देती है, जिसमें IEEE 802.1X जैसे मजबूत प्रमाणीकरण ढांचे, VLANs के माध्यम से तार्किक नेटवर्क विभाजन (logical network segmentation), और Bring Your Own Device (BYOD) एंडपॉइंट्स के सुरक्षित ऑनबोर्डिंग पर ध्यान केंद्रित किया गया है।
विरासत (legacy) प्री-शेयर्ड कीज़ (PSK) से दूर जाकर और पहचान-संचालित एक्सेस नीतियों को अपनाकर, स्वास्थ्य सेवा संगठन उल्लंघन के जोखिम को कम कर सकते हैं, परिचालन संबंधी बाधाओं को कम कर सकते हैं, और डिजिटल परिवर्तन कार्यक्रमों के लिए वायरलेस आधार प्रदान कर सकते हैं। इसका व्यावसायिक पक्ष भी उतना ही मजबूत है: हेल्पडेस्क ओवरहेड में कमी, प्रमाणित DSP टूलकिट अनुपालन, और एक ऐसा नेटवर्क जो बिना किसी पूर्ण बुनियादी ढांचे के पुनर्निर्माण के भविष्य के नैदानिक नवाचारों का समर्थन करने में सक्षम हो।
तकनीकी गहन विश्लेषण
प्रमाणीकरण और एक्सेस नियंत्रण
एक सुरक्षित स्वास्थ्य सेवा वायरलेस नेटवर्क की नींव पहचान-आधारित एक्सेस नियंत्रण है। प्री-शेयर्ड कीज़ का उपयोग करने वाले विरासत WPA2-Personal नेटवर्क नैदानिक वातावरण के लिए मौलिक रूप से अनुपयुक्त हैं। वे कोई व्यक्तिगत जवाबदेही प्रदान नहीं करते हैं, कर्मचारियों के जाने पर ऑनबोर्डिंग हटाने की प्रक्रिया को जटिल बनाते हैं, और क्रेडेंशियल के साथ समझौता होने या इच्छित समूह से बाहर साझा किए जाने पर विफलता का एक एकल बिंदु (single point of failure) पेश करते हैं।
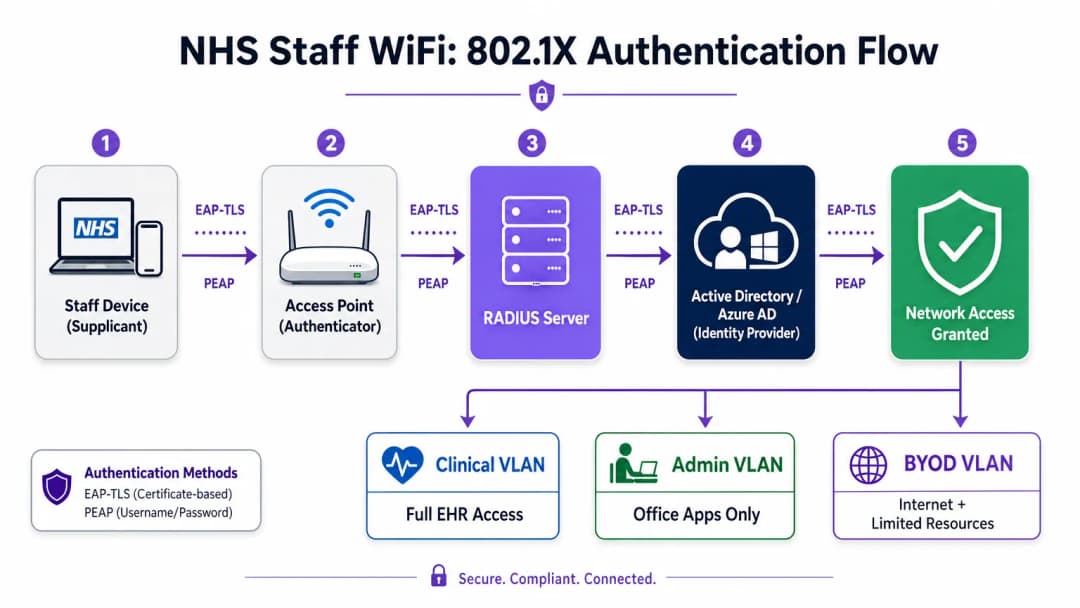
आधुनिक NHS तैनाती में WPA3-Enterprise (या न्यूनतम संक्रमण स्थिति के रूप में WPA2-Enterprise) को IEEE 802.1X प्रमाणीकरण का उपयोग करके अनिवार्य किया जाना चाहिए। इस ढांचे के लिए आवश्यक है कि नेटवर्क एक्सेस दिए जाने से पहले प्रत्येक उपयोगकर्ता या डिवाइस अद्वितीय क्रेडेंशियल प्रस्तुत करे, और उस प्रमाणीकरण का परिणाम यह निर्धारित करता है कि डिवाइस को किस तार्किक नेटवर्क सेगमेंट पर रखा जाए।
स्वास्थ्य सेवा तैनाती में दो EAP तरीके हावी हैं:
| EAP तरीका | प्रमाणीकरण तंत्र | इसके लिए सबसे उपयुक्त | सुरक्षा स्तर |
|---|---|---|---|
| EAP-TLS | क्लाइंट-साइड डिजिटल प्रमाणपत्र | कॉर्पोरेट-प्रबंधित नैदानिक उपकरण | उच्चतम — फ़िशिंग के लिए कोई पासवर्ड नहीं |
| PEAP-MSCHAPv2 | एन्क्रिप्टेड टनल में उपयोगकर्ता नाम/पासवर्ड | BYOD, व्यवस्थापक कर्मचारी, विरासत उपकरण | उच्च — TLS द्वारा सुरक्षित क्रेडेंशियल |
EAP-TLS कॉर्पोरेट उपकरणों के लिए स्वर्ण मानक (gold standard) है। प्रमाणपत्रों को मोबाइल डिवाइस मैनेजमेंट (MDM) प्लेटफॉर्म के माध्यम से वितरित किया जाता है, जिससे ज़ीरो-टच प्रमाणीकरण सक्षम होता है — डिवाइस पृष्ठभूमि में चुपचाप प्रमाणित हो जाता है। PEAP-MSCHAPv2 एक एन्क्रिप्टेड TLS सत्र के भीतर एक्टिव डायरेक्ट्री या एज़्योर AD क्रेडेंशियल को सुरक्षित रूप से टनल करता है, जिससे यह BYOD परिदृश्यों के लिए उपयुक्त हो जाता है जहां प्रमाणपत्र प्रबंधन व्यावहारिक नहीं है।
वायरलेस बुनियादी ढांचे को संगठन के केंद्रीय पहचान प्रदाता (IdP) के साथ एकीकृत करना यह सुनिश्चित करता है कि किसी कर्मचारी का AD खाता अक्षम होने पर एक्सेस स्वचालित रूप से रद्द हो जाए, जो सीधे एक्सेस लाइफसाइकल प्रबंधन के लिए DSP टूलकिट आवश्यकताओं को पूरा करता है।
नेटवर्क विभाजन और ट्रस्ट ज़ोन
भौतिक एक्सेस पॉइंट पूरे अस्पताल के फर्श पर प्रसारण करते हैं, लेकिन तार्किक विभाजन यह सुनिश्चित करता है कि न्यूनतम विशेषाधिकार के सिद्धांत के आधार पर ट्रैफ़िक अलग रहे। स्वास्थ्य सेवा सेटिंग में एक फ्लैट नेटवर्क आर्किटेक्चर एक गंभीर सुरक्षा भेद्यता है, जो एक समझौता किए गए अतिथि डिवाइस या कमजोर IoT सेंसर को संभावित रूप से नैदानिक प्रणालियों तक पहुँचने की अनुमति देता है।
सर्वोत्तम अभ्यास विशिष्ट SSIDs के लिए मैप किए गए अलग वर्चुअल लोकल एरिया नेटवर्क (VLANs) बनाने का निर्देश देता है, जिसमें फ़ायरवॉल नियम उनके बीच ट्रैफ़िक सीमाओं को लागू करते हैं:
| ज़ोन | SSID | प्रमाणीकरण | एक्सेस | QoS प्राथमिकता |
|---|---|---|---|---|
| नैदानिक | NHS-Clinical | EAP-TLS (प्रमाणपत्र) | EHR, PACS, नैदानिक संदेश सेवा | उच्चतम |
| प्रशासनिक | NHS-Staff | PEAP (AD क्रेडेंशियल) | ऑफिस ऐप्स, इंटरनेट | मध्यम |
| मेडिकल IoT | Hidden/MAB | MAC Authentication Bypass | केवल डिवाइस कंट्रोलर | उच्च |
| अतिथि / रोगी | NHS-Guest | Captive Portal | केवल इंटरनेट | निम्न |
| BYOD | NHS-BYOD | PEAP (AD क्रेडेंशियल) | इंटरनेट, सीमित VDI | निम्न |
मेडिकल IoT VLAN विशेष ध्यान देने योग्य है। कई जुड़े हुए चिकित्सा उपकरण — इन्फ्यूजन पंप, रोगी मॉनिटर, वायरलेस कॉल सिस्टम — 802.1X का समर्थन नहीं कर सकते हैं। MAC Authentication Bypass (MAB) इसका विकल्प है, लेकिन इसे सख्त फ़ायरवॉल एक्सेस कंट्रोल लिस्ट (ACLs) के साथ जोड़ा जाना चाहिए जो इन उपकरणों को केवल उनके निर्दिष्ट प्रबंधन सर्वर के साथ संचार करने तक सीमित करते हैं।
BYOD की चुनौती
Bring Your Own Device नीतियां प्रशासनिक कर्मचारियों और आने वाले चिकित्सकों के लिए तेजी से आम हो रही हैं। हालांकि, अप्रबंधित व्यक्तिगत उपकरण एक महत्वपूर्ण जोखिम का प्रतिनिधित्व करते हैं यदि उन्हें विश्वसनीय नेटवर्क सेगमेंट पर जाने की अनुमति दी जाती है।
एक सुरक्षित BYOD तैनाती में इन उपकरणों को एक समर्पित BYOD VLAN पर ऑनबोर्ड करना शामिल है। यह ज़ोन इंटरनेट एक्सेस प्रदान करता है और शायद एक सुरक्षित गेटवे या वर्चुअल डेस्कटॉप इंफ्रास्ट्रक्चर (VDI) के माध्यम से विशिष्ट, गैर-संवेदनशील आंतरिक संसाधनों तक सीमित पहुंच प्रदान करता है। इसमें नैदानिक प्रणालियों या रोगी डेटा स्टोर के लिए सीधे रूटिंग की अनुमति बिल्कुल नहीं होनी चाहिए।

कार्यान्वयन मार्गदर्शिका
एक सुरक्षित NHS स्टाफ WiFi आर्किटेक्चर को तैनात करने के लिए चल रहे नैदानिक संचालन में व्यवधान को कम करने के लिए चरणबद्ध दृष्टिकोण की आवश्यकता होती है।
चरण 1: मूल्यांकन और डिज़ाइन
एक व्यापक वायरलेस साइट सर्वेक्षण के साथ शुरुआत करें। लीड-लाइनेड दीवारों, भारी मशीनरी और घनी आबादी के कारण स्वास्थ्य सेवा वातावरण रेडियो फ्रीक्वेंसी (RF) प्रसार के लिए कुख्यात रूप से कठिन हैं। डिज़ाइन में केवल कवरेज ही नहीं, बल्कि क्षमता का भी ध्यान रखा जाना चाहिए, जिससे आपातकालीन विभागों और बाह्य रोगी क्लीनिकों जैसे उच्च-यातायात वाले क्षेत्रों में पर्याप्त एक्सेस पॉइंट घनत्व सुनिश्चित हो सके।
आवश्यक SSIDs को परिभाषित करें और उन्हें संबंधित VLANs और सुरक्षा नीतियों से मैप करें। प्रसारण SSIDs की संख्या को न्यूनतम रखें — आदर्श रूप से चार से अधिक नहीं — ताकि प्रबंधन ओवरहेड को कम किया जा सके और बीकन फ्रेम कंजेशन को कम किया जा सके, जो समग्र नेटवर्क प्रदर्शन को कम करता है।
चरण 2: बुनियादी ढांचा कॉन्फ़िगरेशन
परिभाषित VLANs का समर्थन करने के लिए कोर स्विचिंग और रूटिंग बुनियादी ढांचे को कॉन्फ़िगर करें। न्यूनतम विशेषाधिकार लागू करने के लिए सेगमेंट के बीच की सीमाओं पर फ़ायरवॉल नियम लागू करें। RADIUS सर्वर (जैसे, Cisco ISE, Aruba ClearPass, या क्लाउड-आधारित RADIUS-as-a-Service) सेट करें और इसे केंद्रीय पहचान प्रदाता के साथ एकीकृत करें। जिन वातावरणों में Purple का प्लेटफ़ॉर्म तैनात है, वहां इस चरण में WiFi Analytics को एकीकृत करना नेटवर्क उपयोग, रोमिंग पैटर्न और क्षमता हॉटस्पॉट में दृश्यता प्रदान करता है।
चरण 3: नीति प्रवर्तन और ऑनबोर्डिंग
प्रमाणीकरण नीतियां तैनात करें। कॉर्पोरेट उपकरणों के लिए, आवश्यक वायरलेस प्रोफाइल और क्लाइंट प्रमाणपत्र (EAP-TLS के लिए) भेजने के लिए MDM समाधान का उपयोग करें। यह सुनिश्चित करता है कि प्रबंधित उपकरण उपयोगकर्ता के हस्तक्षेप के बिना स्वचालित रूप से और सुरक्षित रूप से कनेक्ट हों।
BYOD के लिए, एक स्पष्ट ऑनबोर्डिंग वर्कफ़्लो स्थापित करें — आमतौर पर एक ऑनबोर्डिंग पोर्टल जो उपयोगकर्ता को उनके कॉर्पोरेट क्रेडेंशियल के साथ प्रमाणित करने, स्वीकार्य उपयोग नीति को स्वीकार करने और डिवाइस को सुरक्षित BYOD VLAN पर ले जाने के माध्यम से मार्गदर्शन करता है। Purple के Guest WiFi प्लेटफ़ॉर्म को रोगी और अतिथि SSID के लिए Captive Portal परत के रूप में तैनात किया जा सकता है, जो बड़े पैमाने पर GDPR-अनुरूप डेटा कैप्चर और शर्तों की स्वीकृति को संभालता है।
चरण 4: परीक्षण और सत्यापन
गो-लाइव से पहले, प्रत्येक प्रमाणीकरण पथ, VLAN असाइनमेंट और फ़ायरवॉल नियम का एंड-टू-एंड परीक्षण करें। विशेष रूप से पुनः प्रमाणीकरण घटनाओं की निगरानी करते हुए एक परीक्षण डिवाइस के साथ नैदानिक फर्श पर चलकर रोमिंग व्यवहार को मान्य करें। पुष्टि करें कि फास्ट रोमिंग प्रोटोकॉल (802.11r और 802.11k) सही ढंग से काम कर रहे हैं और एप्लिकेशन सत्र AP संक्रमणों के बाद भी बने रहते हैं।
सर्वोत्तम अभ्यास
प्री-शेयर्ड कीज़ को समाप्त करें। व्यक्तिगत जवाबदेही और केंद्रीकृत एक्सेस नियंत्रण सुनिश्चित करने के लिए सभी कर्मचारियों और नैदानिक नेटवर्क को 802.1X प्रमाणीकरण पर स्थानांतरित करें। यह DSP टूलकिट अनुपालन के लिए एक गैर-परक्राम्य आवश्यकता है।
सख्त विभाजन लागू करें। अतिथि, BYOD, या IoT ट्रैफ़िक को कभी भी नैदानिक डेटा के समान तार्किक सेगमेंट पर अनुमति न दें। डिफ़ॉल्ट नीति के रूप में स्पष्ट अस्वीकार (deny) नियमों के साथ, इंटर-VLAN रूटिंग को नियंत्रित करने के लिए स्टेटफुल फ़ायरवॉल का उपयोग करें।
नैदानिक ट्रैफ़िक को प्राथमिकता दें। विशेष रूप से उच्च भीड़ की अवधि के दौरान, अतिथि या प्रशासनिक ट्रैफ़िक की तुलना में नैदानिक अनुप्रयोगों — वॉयस ओवर WLAN, EHR एक्सेस — को प्राथमिकता देने के लिए वायरलेस कंट्रोलर और स्विच पर QoS नीतियां लागू करें।
फास्ट रोमिंग सक्षम करें। 802.11r (फास्ट BSS ट्रांज़िशन) और 802.11k (रेडियो रिसोर्स मेजरमेंट) को तैनात करें ताकि यह सुनिश्चित हो सके कि नैदानिक कर्मचारी एप्लिकेशन टाइमआउट या टूटे हुए कनेक्शन का अनुभव किए बिना सुविधा के माध्यम से आगे बढ़ सकें।
निरंतर निगरानी। नेटवर्क स्वास्थ्य की निगरानी करने, अनधिकृत एक्सेस पॉइंट की पहचान करने और उपयोगकर्ता रोमिंग व्यवहार को ट्रैक करने के लिए एनालिटिक्स प्लेटफॉर्म का उपयोग करें। फुटफॉल और उपयोग के पैटर्न को समझना — Retail और Hospitality वातावरण में सिद्ध एक तकनीक — क्षमता योजना और समस्या निवारण के लिए अस्पताल की सेटिंग में भी उतनी ही मूल्यवान है।
नियमित ऑडिटिंग। जहां लागू हो, DSP टूलकिट, साइबर एसेंशियल प्लस और ISO 27001 के साथ निरंतर अनुपालन सुनिश्चित करने के लिए वार्षिक वायरलेस जोखिम मूल्यांकन आयोजित करें।
समस्या निवारण और जोखिम शमन
प्रमाणीकरण टाइमआउट
उच्च क्लाइंट घनत्व वाले वातावरण में, RADIUS सर्वर अभिभूत हो सकते हैं, जिससे प्रमाणीकरण टाइमआउट और टूटे हुए कनेक्शन हो सकते हैं। सुनिश्चित करें कि RADIUS बुनियादी ढांचा पर्याप्त रूप से स्केल किया गया है और अत्यधिक उपलब्ध है। कई प्रमाणीकरण सर्वरों में लोड बैलेंसिंग लागू करें और एक प्रमुख परिचालन मीट्रिक के रूप में RADIUS प्रतिक्रिया समय की निगरानी करें।
रोमिंग के मुद्दे
वार्डों के बीच तेजी से चलने वाले नैदानिक कर्मचारियों को टूटे हुए कनेक्शन का अनुभव हो सकता है यदि वायरलेस बुनियादी ढांचा फास्ट रोमिंग प्रोटोकॉल का समर्थन नहीं करता है। वायरलेस कंट्रोलर पर 802.11r और 802.11k सक्षम करें और सुनिश्चित करें कि क्लाइंट डिवाइस इन मानकों का समर्थन करते हैं। कवरेज अंतराल या 'स्टिकी क्लाइंट' मुद्दों की पहचान करने और उन्हें हल करने के लिए पोस्ट-डिप्लॉयमेंट रोमिंग सर्वेक्षण आयोजित करें, जहां एक डिवाइस करीब जाने के बजाय दूर के, कमजोर AP से चिपका रहता है।
विरासत डिवाइस असंगतता
पुराने चिकित्सा उपकरण WPA3 या 802.1X जैसे आधुनिक सुरक्षा प्रोटोकॉल का समर्थन नहीं कर सकते हैं। MAB का उपयोग करके इन उपकरणों को एक समर्पित IoT VLAN पर अलग करें। उनके संचार को केवल आवश्यक प्रबंधन सर्वर तक सीमित करने के लिए सख्त फ़ायरवॉल नियम लागू करें। उन महत्वपूर्ण उपकरणों के लिए हार्डवेयर अपग्रेड या वायरलेस ब्रिज पर विचार करें जिन्हें मूल रूप से सुरक्षित नहीं किया जा सकता है।
प्रमाणपत्र की समाप्ति
EAP-TLS तैनाती परिभाषित समाप्ति अवधि वाले प्रमाणपत्रों पर निर्भर करती है। यदि प्रमाणपत्र नवीनीकरण के बिना समाप्त हो जाते हैं, तो डिवाइस प्रमाणित करने में विफल हो जाएंगे, जिससे व्यापक नैदानिक व्यवधान होगा। MDM प्लेटफॉर्म के माध्यम से SCEP (सिंपल सर्टिफिकेट एनरोलमेंट प्रोटोकॉल) के माध्यम से स्वचालित प्रमाणपत्र नवीनीकरण लागू करें, और सक्रिय रूप से प्रमाणपत्र समाप्ति तिथियों की निगरानी करें।
ROI और व्यावसायिक प्रभाव
एक सुरक्षित, एंटरप्राइज़-ग्रेड वायरलेस आर्किटेक्चर में निवेश नैदानिक, परिचालन और IT डोमेन में मापने योग्य रिटर्न प्रदान करता है।
नैदानिक दक्षता। विश्वसनीय कनेक्टिविटी यह सुनिश्चित करती है कि चिकित्सकों के पास देखभाल के बिंदु पर रोगी के रिकॉर्ड तक तत्काल पहुंच हो, जिससे जानकारी खोजने या टूटे हुए कनेक्शन से निपटने में लगने वाला समय कम हो जाता है। यह सीधे रोगी थ्रूपुट और देखभाल वितरण की गुणवत्ता को प्रभावित करता है।
कम IT ओवरहेड। साझा पासवर्ड और मैन्युअल ऑनबोर्डिंग से हटकर स्वचालित, प्रमाणपत्र-आधारित प्रमाणीकरण की ओर बढ़ने से पासवर्ड रीसेट और कनेक्टिविटी समस्याओं से संबंधित हेल्पडेस्क टिकटों में काफी कमी आती है। एक NHS ट्रस्ट ने 802.1X पर माइग्रेशन के बाद वायरलेस से संबंधित हेल्पडेस्क कॉल में 40% की कमी दर्ज की।
जोखिम शमन। सख्त विभाजन और मजबूत प्रमाणीकरण DSP टूलकिट आवश्यकताओं को पूरा करने, डेटा उल्लंघनों या अनुपालन विफलताओं से जुड़े वित्तीय और प्रतिष्ठित जोखिमों को कम करने के लिए मौलिक हैं। डेटा उल्लंघन की लागत उचित रूप से तैयार की गई वायरलेस संपत्ति में निवेश से कहीं अधिक है।
भविष्य के लिए तैयार करना (Future-Proofing)। एक अच्छी तरह से डिज़ाइन किया गया वायरलेस नेटवर्क भविष्य की डिजिटल स्वास्थ्य पहलों — स्थान-आधारित सेवाएं, रीयल-टाइम एसेट ट्रैकिंग, उन्नत टेलीहेल्थ एप्लिकेशन — के लिए आधार प्रदान करता है, जो Healthcare और Transport जैसे संबंधित क्षेत्रों में व्यापक रणनीतिक लक्ष्यों के साथ संरेखित होता है जहां मोबाइल कनेक्टिविटी परिचालन दक्षता को रेखांकित करती है।
उन संगठनों के लिए जो यह समझना चाहते हैं कि Purple का प्लेटफ़ॉर्म इस आर्किटेक्चर के अतिथि और रोगी WiFi परत से कैसे मेल खाता है, Healthcare उद्योग पृष्ठ NHS-संगत Captive Portal, एनालिटिक्स और GDPR-अनुरूप डेटा हैंडलिंग क्षमताओं का एक विस्तृत अवलोकन प्रदान करता है। वही एनालिटिक्स सिद्धांत जो Retail में ग्राहक जुड़ाव को बढ़ावा देते हैं, सीधे अस्पताल संपदा टीमों के लिए परिचालन खुफिया में अनुवादित होते हैं।
Key Definitions
IEEE 802.1X
An IEEE standard for port-based Network Access Control (PNAC). It provides an authentication mechanism to devices wishing to attach to a LAN or WLAN, requiring each device to present credentials before being granted access.
This is the mandatory standard for replacing insecure shared passwords with individual, identity-based logins for staff and clinical devices. It is the cornerstone of a DSP Toolkit-compliant wireless architecture.
VLAN (Virtual Local Area Network)
A logical subnetwork that groups a collection of devices from different physical network segments. VLANs allow network administrators to partition a single switched network to match the functional and security requirements of different user groups.
VLANs are essential for segmenting clinical traffic from guest and administrative traffic, limiting the blast radius of a potential security breach and enforcing the principle of least privilege.
RADIUS (Remote Authentication Dial-In User Service)
A networking protocol that provides centralised Authentication, Authorisation, and Accounting (AAA) management for users who connect and use a network service.
The RADIUS server acts as the decision engine between the wireless access points and the central identity database (Active Directory), deciding who gets access and to which VLAN they are assigned.
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
An EAP method that relies on client and server certificates to establish a secure, mutually authenticated connection. Neither party trusts the other without a valid certificate.
The most secure method for authenticating hospital-owned devices. Certificates distributed via MDM ensure that only managed, trusted endpoints can access the clinical network, with no password to phish or share.
MAB (MAC Authentication Bypass)
A method of authenticating devices based on their hardware MAC address, used as a fallback for devices that do not support 802.1X.
Necessary for legacy medical IoT devices that need network access but cannot handle complex authentication protocols. Must always be paired with strict firewall ACLs to contain the device to its permitted communication paths.
DSP Toolkit (Data Security and Protection Toolkit)
An online self-assessment tool mandated by NHS England that all organisations must complete if they have access to NHS patient data and systems. It maps to the National Data Guardian's ten data security standards.
Compliance with the DSP Toolkit is mandatory for NHS organisations and their suppliers. Robust wireless security — including 802.1X, segmentation, and access lifecycle management — is a critical component of demonstrating compliance.
SSID (Service Set Identifier)
The primary name associated with an 802.11 wireless local area network, broadcast by access points to allow client devices to identify and connect to the network.
Hospitals should minimise the number of broadcast SSIDs (e.g., NHS-Clinical, NHS-Guest) to reduce management overhead and RF overhead. Each SSID should map to a specific security policy and VLAN.
QoS (Quality of Service)
Technologies that manage data traffic to reduce packet loss, latency, and jitter on a network by prioritising certain types of traffic over others.
Crucial in healthcare to ensure that life-critical clinical applications and voice communications are always prioritised over less important traffic such as guest video streaming or software updates.
802.11r (Fast BSS Transition)
An IEEE amendment that enables fast roaming between access points by pre-authenticating the client to the target AP before the physical transition occurs, dramatically reducing roaming latency.
Essential for clinical environments where staff are constantly moving. Without 802.11r, devices must perform a full RADIUS re-authentication on every AP transition, which can cause application sessions to time out.
Worked Examples
An NHS Trust is deploying new mobile workstations (Workstations on Wheels) across multiple wards. The IT team needs to ensure these devices maintain connectivity as nurses move between access points, while also guaranteeing that only authorised devices can access the clinical VLAN containing the Electronic Health Record system.
The Trust should implement an 802.1X authentication framework using EAP-TLS. The IT team will use their MDM solution to push a unique client certificate and the corresponding wireless profile to each workstation. The wireless controllers will be configured to authenticate these devices against a RADIUS server, which verifies the certificate against the internal PKI. Upon successful authentication, the RADIUS server dynamically assigns the workstation to the dedicated Clinical VLAN via a RADIUS attribute (e.g., Tunnel-Private-Group-ID). To address the roaming requirement, 802.11r (Fast BSS Transition) and 802.11k (Radio Resource Measurement) must be enabled on the wireless infrastructure to allow the workstations to transition seamlessly between access points without performing a full re-authentication cycle against the RADIUS server each time.
A hospital needs to provide internet access for visiting locum doctors using their personal laptops (BYOD). These doctors need to access cloud-based medical reference tools but must be strictly prohibited from accessing the hospital's internal patient databases.
The hospital should deploy a dedicated BYOD SSID mapped to an isolated BYOD VLAN. Authentication should be handled via 802.1X using PEAP-MSCHAPv2, allowing the locums to log in using temporary Active Directory credentials provided by HR upon arrival. The core firewall must be configured with an ACL that explicitly denies any routing from the BYOD VLAN to the Clinical or Administrative VLANs, permitting only outbound traffic to the internet. Additionally, a captive portal can be utilised upon initial connection to enforce an Acceptable Use Policy before granting full internet access. When the locum's temporary AD account is disabled at the end of their engagement, their wireless access is automatically revoked.
Practice Questions
Q1. A new wing is being added to the hospital, and the facilities team wants to deploy wireless temperature sensors in the medication storage fridges. These sensors only support WPA2-Personal (Pre-Shared Key) and cannot use 802.1X. How should the network architect integrate these securely?
Hint: Consider the principle of least privilege and how to isolate non-compliant devices from clinical systems.
View model answer
The architect should create a dedicated, hidden SSID mapped to a specific 'Facilities IoT' VLAN. The sensors will connect using the PSK. Crucially, strict firewall ACLs must be applied to this VLAN, allowing the sensors to communicate only with their specific central management server and denying all other traffic — particularly routing to the Clinical VLAN or the internet. MAC Authentication Bypass (MAB) should also be configured to ensure only the specific MAC addresses of the purchased sensors are permitted on that VLAN, preventing rogue devices from joining using the same PSK.
Q2. During a busy morning shift, nurses report that their tablets are frequently dropping connection to the EHR system as they walk the length of the ward, requiring them to log in again. The wireless coverage survey shows strong signal strength throughout the ward. What is the likely cause and solution?
Hint: Strong signal does not guarantee seamless transitions between access points. Consider the authentication overhead on each AP transition.
View model answer
The likely cause is a lack of fast roaming protocols. As the tablet moves out of range of one AP and connects to the next, it is being forced to perform a full 802.1X re-authentication against the RADIUS server, which introduces enough latency to cause the EHR application session to time out. The solution is to enable 802.11r (Fast BSS Transition) on the wireless controllers, which allows the client to securely roam between APs without the latency of a full re-authentication cycle. 802.11k should also be enabled to help the device identify the optimal target AP before the transition occurs.
Q3. An NHS Trust is preparing for its annual DSP Toolkit assessment. The auditor notes that the administrative staff use a shared password to access the Staff WiFi network. What is the primary risk identified here, and what is the recommended remediation?
Hint: Focus on individual accountability and the access lifecycle when staff leave the organisation.
View model answer
The primary risk is a lack of individual accountability and poor access lifecycle management. If an administrative staff member leaves the Trust, the shared password remains valid, potentially allowing unauthorised access. Furthermore, it is impossible to audit which specific user performed an action on the network. The remediation is to deprecate the shared password (PSK) network and migrate administrative staff to an 802.1X authenticated network using PEAP-MSCHAPv2 with their Active Directory credentials. This ensures individual accountability and automatic access revocation when their AD account is disabled upon leaving, directly addressing the DSP Toolkit's requirements for access control and audit logging.
Continue reading in this series
Understanding Cisco SUDI: Hardware-Anchored Identity in Secure Network Access Control
This guide explains how Cisco SUDI provides hardware-anchored, cryptographically secure identity for enterprise network infrastructure. Learn how to replace spoofable MAC addresses with immutable 802.1AR certificates to secure your venue's network access control.
How to Configure SCEP for Automated Enterprise WiFi Certificate Enrollment
This guide explains how to configure SCEP (Simple Certificate Enrollment Protocol) for automated enterprise WiFi certificate enrollment, covering the full architecture from PKI and NDES through to MDM profile deployment and RADIUS validation. It is aimed at IT managers, network architects, and CTOs at hotels, retail chains, stadiums, conference centres, and public-sector organisations who need to move beyond pre-shared keys and implement scalable, identity-based 802.1X EAP-TLS authentication. Purple's hardware-agnostic, cloud overlay platform integrates directly with this architecture, providing the guest and BYOD WiFi layer that sits alongside your certificate-authenticated staff network.
How to Implement SCEP for Automated WiFi Certificate Enrollment
This guide explains how to implement SCEP (Simple Certificate Enrollment Protocol) for automated WiFi certificate enrollment across enterprise venues. It covers the full architectural blueprint - from PKI design and MDM integration to the mandatory three-step deployment sequence - and shows IT managers and network architects how to eliminate shared credentials, automate certificate lifecycle management, and satisfy PCI DSS and GDPR requirements at scale.