Patient WiFi: Una Guida Completa per gli NHS Trusts e gli Operatori Ospedalieri
Una guida tecnica e commerciale definitiva per gli NHS Trusts e gli operatori ospedalieri sulla distribuzione, la sicurezza e la monetizzazione del Patient WiFi. Tratta la segmentazione della rete, la conformità DSPT, il filtraggio dei contenuti e l'utilizzo dell'analisi per migliorare i risultati per i pazienti.
Ascolta questa guida
Visualizza trascrizione del podcast

Riepilogo Esecutivo
Fornire un Patient WiFi robusto, sicuro e conforme non è più un servizio "opzionale" per gli NHS Trusts e gli operatori ospedalieri privati, ma un requisito infrastrutturale critico. I pazienti si aspettano connettività per gestire le proprie vite, comunicare con la famiglia e accedere ai servizi sanitari digitali durante la loro degenza. Tuttavia, fornire questa connettività in un ambiente clinico introduce significative sfide tecniche e di governance.
Questa guida fornisce un quadro completo per i responsabili IT, gli architetti di rete e i CTO per progettare, implementare e gestire le reti Patient WiFi. Esploriamo la necessità di una rigorosa segmentazione della rete, le complessità della conformità al Data Security and Protection Toolkit (DSPT), l'implementazione di un rigoroso filtraggio dei contenuti e i modelli commerciali che sostengono queste implementazioni. Trattando il Patient WiFi come un servizio di livello enterprise piuttosto che come un overlay di banda larga consumer, gli NHS Trusts possono mitigare i rischi, garantire l'integrità dei sistemi clinici e sfruttare piattaforme come Guest WiFi per acquisire informazioni utili e migliorare la soddisfazione dei pazienti.
Approfondimento Tecnico: Architettura e Standard
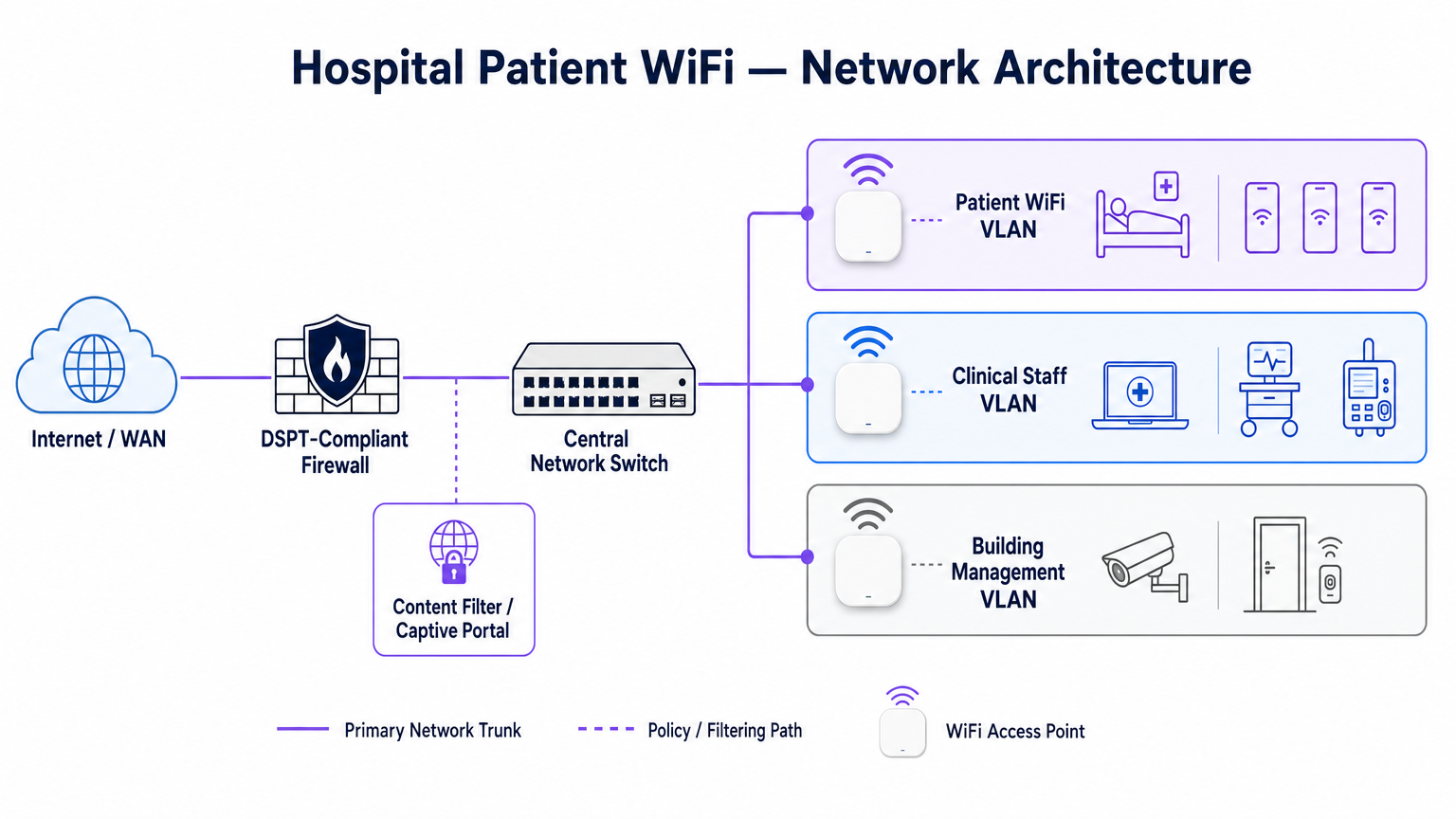
La base di qualsiasi implementazione WiFi ospedaliera è l'assoluta segregazione tra il traffico dei pazienti e i sistemi clinici. Un ospedale è un ambiente RF ad alta densità e alta interferenza dove dispositivi critici per la vita operano in stretta prossimità con gli smartphone consumer.
Segmentazione della Rete e Progettazione VLAN
Per proteggere l'integrità clinica, il Patient WiFi deve operare su una Virtual Local Area Network (VLAN) dedicata. L'architettura enterprise standard prevede un minimo di tre segmenti distinti:
- VLAN Pazienti/Ospiti: Instrada attraverso un captive portal, impone un rigoroso filtraggio dei contenuti e fornisce accesso solo a internet.
- VLAN Clinica: Dedicata ai dispositivi del personale e alle apparecchiature mediche (es. pompe per infusione, workstation mobili). Bypassa il captive portal e instrada attraverso un percorso monitorato e sicuro.
- VLAN Gestione Edificio: Supporta dispositivi IoT, CCTV e controlli ambientali.
Il traffico sulla VLAN Pazienti deve essere isolato a livello di switch e limitato da regole firewall che neghino esplicitamente l'instradamento verso le sottoreti interne.
Densità degli Access Point e Pianificazione RF
L'implementazione del WiFi in un ospedale richiede il superamento di significative barriere fisiche: pareti rivestite di piombo, macchinari pesanti e cemento denso. Affidarsi alla "copertura del corridoio" è una modalità di fallimento comune.
Un'indagine RF predittiva, seguita da una convalida attiva post-installazione, è obbligatoria.
Per le nuove implementazioni, IEEE 802.11ax (Wi-Fi 6) è lo standard di riferimento. La sua implementazione di Orthogonal Frequency-Division Multiple Access (OFDMA) e BSS Colouring è cruciale per gestire l'alta densità di dispositivi tipica dei moderni reparti ospedalieri, riducendo la latenza e mitigando le interferenze dai sistemi di telemetria medica che operano nella banda a 2.4 GHz.
Requisiti di Backhaul e Throughput
Un errore comune è il provisioning di access point di livello enterprise ma con un backhaul insufficiente. Un ospedale da 500 posti letto può facilmente generare 1 Gbps di domanda concorrente durante le ore di punta serali. Gli operatori devono fornire linee dedicate e non contese piuttosto che circuiti a banda larga condivisi per garantire il throughput ed evitare di creare colli di bottiglia nella rete centrale. Per ulteriori informazioni sulla connettività dedicata, consultare Cos'è una Linea Dedicata? Internet Aziendale Dedicato .
Guida all'Implementazione: Conformità e Filtraggio
L'implementazione dell'infrastruttura fisica è solo metà della sfida; l'overlay di governance e conformità è altrettanto critico.
Conformità DSPT
Per gli NHS Trusts, l'adesione al Data Security and Protection Toolkit (DSPT) non è negoziabile. Le implementazioni Patient WiFi devono dimostrare:
- Rigorosa segmentazione della rete.
- Robusti controlli di accesso e registrazione degli audit (log di connessione conservati per un minimo di 12 mesi).
- Test di penetrazione annuali da parte di terzi.
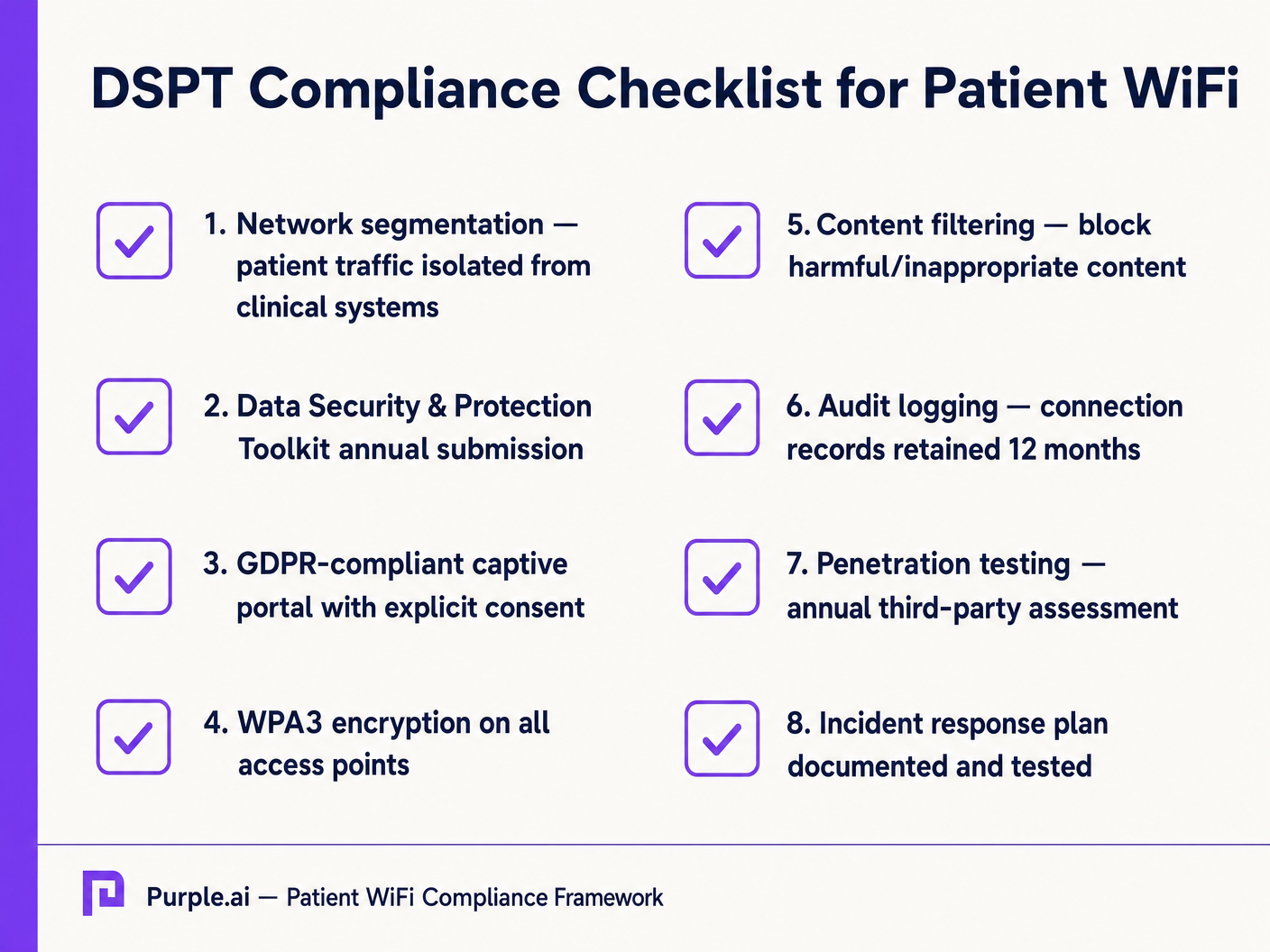
Filtraggio dei Contenuti
Le linee guida dell'NHS impongono che il Patient WiFi debba bloccare l'accesso a contenuti inappropriati o dannosi, inclusi materiale per adulti, siti estremisti e piattaforme di gioco d'azzardo. Ciò si ottiene tipicamente tramite filtraggio basato su DNS o proxy applicato direttamente alla VLAN Pazienti. La soluzione di filtraggio deve acquisire feed di intelligence sulle minacce in tempo reale per bloccare dinamicamente i domini dannosi di nuova identificazione.
Captive Portals e GDPR
Il captive portal è il gateway alla rete e il meccanismo primario per acquisire il consenso dell'utente. Ai sensi del GDPR, gli NHS Trusts devono ottenere un consenso esplicito e informato prima di elaborare dati personali (come indirizzi MAC o indirizzi email). Il portale deve presentare una chiara politica sulla privacy e opt-in espliciti. L'utilizzo di una piattaforma robusta garantisce la conformità consentendo al contempo la raccolta di preziosi dati demografici.
ROI e Impatto Commerciale: Modelli Gratuiti vs. a Pagamento
La strategia commerciale dietro il Patient WiFi definisce la sua sostenibilità a lungo termine.
Il Modello WiFi Gratuito
La stragrande maggioranza degli NHS Trusts offre Patient WiFi gratuitamente al punto di utilizzo. Questo modello è tipicamente finanziato tramite spese in conto capitale o budget operativi. Il ROI è misurato in soddisfazione del paziente (spesso riflessa in Frienpunteggi dei test per pazienti e familiari) e la riduzione dell'onere amministrativo per il personale clinico, che non deve più gestire reclami relativi alla connettività.
Il Modello Concessionario
Alcuni Trust più grandi adottano un modello concessionario, in cui un fornitore di servizi gestiti (MSP) di terze parti finanzia l'infrastruttura in cambio di diritti di monetizzazione. Ciò può comportare la pubblicazione di annunci mirati tramite il Captive Portal o l'offerta di un servizio a più livelli (navigazione base gratuita, streaming premium a pagamento). Se adottano questo modello, i Trust devono assicurarsi che il contenuto pubblicitario sia rigorosamente controllato per allinearsi ai valori del NHS e che le pratiche di monetizzazione dei dati siano conformi al GDPR.
Integrando WiFi Analytics , i Trust possono monitorare l'utilizzo della rete, tracciare i tempi di permanenza dei pazienti e attivare sondaggi di feedback automatizzati dopo la connessione, trasformando un centro di costo in una risorsa strategica per il miglioramento operativo. Questo approccio basato sui dati rispecchia implementazioni di successo in altri settori, come Healthcare e Retail .
Definizioni chiave
VLAN (Virtual Local Area Network)
A logical subnetwork that groups a collection of devices from different physical LANs. Essential for isolating patient traffic from clinical systems.
Used by network architects to ensure that a compromised patient device cannot access sensitive medical equipment or electronic health records.
DSPT (Data Security and Protection Toolkit)
An online self-assessment tool that allows NHS organisations to measure their performance against the National Data Guardian's 10 data security standards.
Mandatory for all NHS Trusts; failure to properly segment patient WiFi or log access can result in a failed DSPT submission.
Captive Portal
A web page that a user of a public-access network is obliged to view and interact with before access is granted.
The primary interface for capturing user consent, presenting terms of use, and applying brand identity to the WiFi experience.
802.11ax (Wi-Fi 6)
The sixth generation of the Wi-Fi standard, designed specifically to improve performance in high-density environments.
Crucial for hospital wards where dozens of patients, visitors, and staff devices are competing for airtime simultaneously.
OFDMA (Orthogonal Frequency-Division Multiple Access)
A feature of Wi-Fi 6 that allows a single transmission to deliver data to multiple devices simultaneously.
Reduces latency and improves efficiency in crowded hospital environments, preventing the network from grinding to a halt during peak hours.
Content Filtering
The use of software or hardware to restrict the content that a reader is authorised to access over the network.
Required by NHS guidance to prevent access to illegal, extremist, or adult content on patient networks.
Leased Line
A dedicated, fixed-bandwidth, symmetric data connection connecting a business directly to the internet exchange.
Necessary for hospital WiFi backhaul to ensure guaranteed throughput, avoiding the contention issues of shared broadband.
MAC Address
A unique identifier assigned to a network interface controller (NIC) for use as a network address in communications.
Considered personal data under GDPR; its collection and storage by the WiFi analytics platform requires explicit user consent.
Esempi pratici
A 400-bed NHS Trust is experiencing severe network congestion on its legacy patient WiFi during the hours of 6 PM to 9 PM, leading to patient complaints and staff distraction. The current setup uses a shared 500 Mbps broadband connection and Wi-Fi 4 (802.11n) access points in the corridors.
- Upgrade backhaul to a dedicated 1 Gbps symmetrical leased line to guarantee peak-hour throughput. 2. Replace corridor-based Wi-Fi 4 APs with in-room Wi-Fi 6 (802.11ax) APs to improve RF penetration and handle high device density via OFDMA. 3. Implement traffic shaping on the firewall to cap individual user bandwidth at 5 Mbps, preventing single users from monopolising the connection with 4K streaming.
A private hospital group wants to deploy a new patient WiFi network but is concerned about the DSPT compliance implications of capturing patient data on the captive portal.
Deploy a GDPR-compliant captive portal solution (like Purple) that separates authentication data from clinical data. Configure the portal to require explicit opt-in for any data processing beyond the minimum required for network access. Ensure the Patient VLAN is strictly isolated from the Clinical VLAN via the core firewall. Implement DNS-based content filtering to block malicious and inappropriate categories.
Domande di esercitazione
Q1. An NHS Trust wants to implement a single SSID for both staff and patients to 'simplify the user experience'. They plan to use a captive portal to differentiate user types. Is this approach recommended?
Suggerimento: Consider the DSPT requirements for network segmentation and the risk of a compromised patient device.
Visualizza risposta modello
No, this approach is highly discouraged and introduces significant security risks. Patient and clinical staff traffic must be segregated at the VLAN level with separate SSIDs. Relying solely on a captive portal for differentiation does not provide adequate Layer 2 isolation, putting clinical systems at risk from malware or lateral movement originating from untrusted patient devices.
Q2. A hospital is planning to upgrade its patient WiFi and wants to ensure adequate coverage. The IT manager suggests placing access points in the main corridors to cover the adjacent patient rooms and save on hardware costs. What is the flaw in this plan?
Suggerimento: Think about the physical construction of hospital environments and RF attenuation.
Visualizza risposta modello
Corridor placement is a flawed strategy in hospitals. Hospital walls often contain lead lining (for X-ray rooms), heavy concrete, and dense infrastructure that severely attenuates RF signals. This results in poor in-room coverage, high latency, and dropped connections. Access points should be deployed inside patient rooms or wards based on a professional predictive RF survey.
Q3. A Trust has deployed patient WiFi but is receiving complaints about slow speeds during the evening. The APs are Wi-Fi 6, and the core switches are 10G capable. The internet connection is a 1 Gbps shared broadband line. What is the likely bottleneck?
Suggerimento: Differentiate between local network capacity and WAN backhaul.
Visualizza risposta modello
The bottleneck is the shared broadband internet connection. Even with high-capacity local infrastructure (Wi-Fi 6 and 10G switches), a shared broadband line suffers from contention ratios, meaning the bandwidth is shared with other premises in the area. During evening peak hours, this contention severely degrades throughput. The Trust should upgrade to a dedicated, uncontended leased line.
Continua a leggere questa serie
Cos'è una Probe Request? Capire come i dispositivi scoprono le reti
Questa guida di riferimento tecnico offre un'analisi approfondita delle probe request IEEE 802.11, della scansione attiva versus passiva e dell'impatto della randomizzazione MAC sull'analisi dei dati dei luoghi. Fornisce strategie di implementazione attuabili per gli architetti di rete al fine di ottimizzare le implementazioni ad alta densità, mitigare le probe storm e garantire una raccolta dati accurata e conforme al GDPR utilizzando livelli di identità autenticati.
Come Risolvere il WiFi Lento Senza Aggiornare il Tuo Piano Internet
Una guida tecnica di riferimento completa per IT managers e network architects sull'ottimizzazione delle prestazioni WiFi aziendali senza aumentare la ISP bandwidth. Copre RF tuning, la gestione della densità dei client, l'implementazione di QoS e come sfruttare WiFi analytics per diagnosticare e risolvere i colli di bottiglia.
La Checklist per la Migrazione da NAC Legacy a NAC Cloud-Native
Questa guida tecnica di riferimento autorevole fornisce una checklist strutturata in tre fasi per la migrazione da Network Access Control (NAC) legacy a un'architettura cloud-native. Fornisce a manager IT e architetti di rete strategie attuabili per gestire l'integrazione dell'identità, la parità delle policy e la conformità senza interrompere le operazioni della sede.