हेल्थकेयर के लिए NAC: मेडिकल उपकरणों और रोगी डेटा को सुरक्षित करना
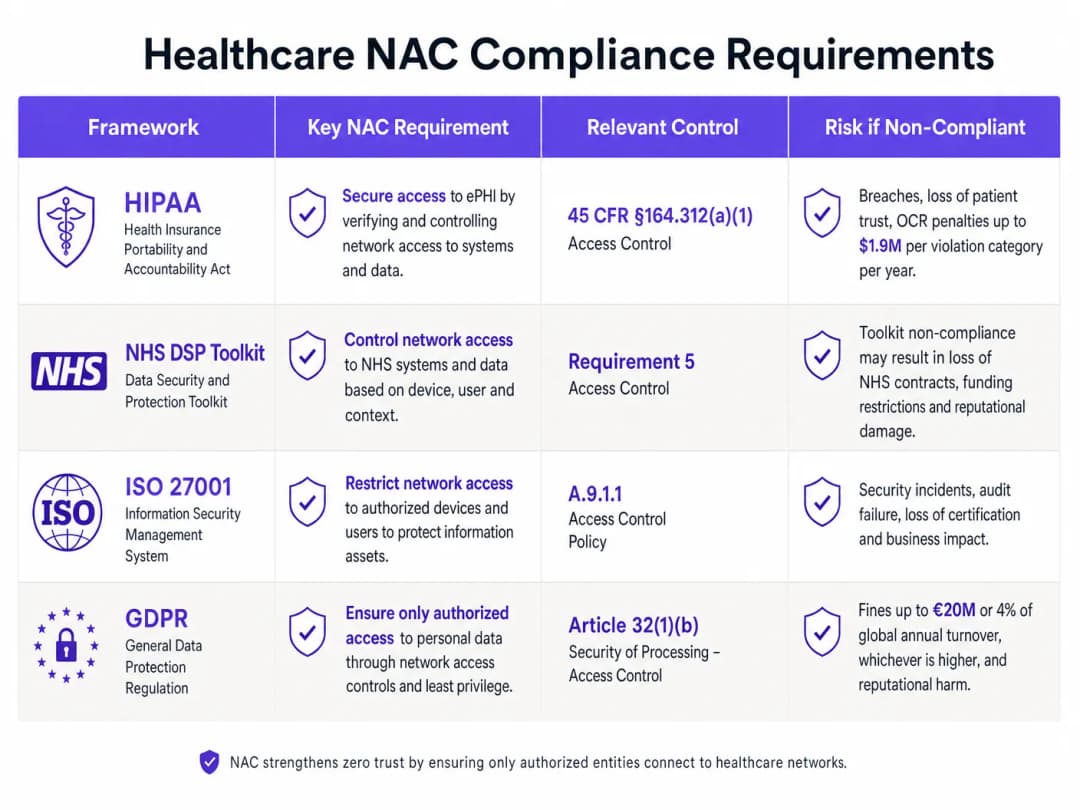
यह गाइड हेल्थकेयर परिवेशों में नेटवर्क एक्सेस कंट्रोल (NAC) को तैनात करने के लिए एक व्यापक तकनीकी संदर्भ प्रदान करती है, जिसमें मेडिकल IoT, क्लिनिकल सिस्टम और गेस्ट एक्सेस के लिए आर्किटेक्चर डिज़ाइन, ऑथेंटिकेशन मैकेनिज्म, डिवाइस प्रोफाइलिंग और VLAN सेगमेंटेशन शामिल है। यह HIPAA, NHS DSP Toolkit, ISO 27001 और GDPR के अनुपालन आवश्यकताओं को संबोधित करता है, जिसमें ठोस कार्यान्वयन परिदृश्य और वेंडर-न्यूट्रल सर्वोत्तम अभ्यास शामिल हैं। हेल्थकेयर में IT निदेशकों और CTOs के लिए, क्लिनिकल वर्कफ़्लो को बाधित किए बिना मेडिकल उपकरणों और रोगी डेटा को सुरक्षित करने का यह एक परिचालन ब्लूप्रिंट है।
इस गाइड को सुनें
पॉडकास्ट ट्रांसक्रिप्ट देखें
📚 हमारी मुख्य श्रृंखला का हिस्सा: Enterprise WiFi Security Guide →

कार्यकारी सारांश (Executive Summary)
एक आधुनिक हेल्थकेयर नेटवर्क को सुरक्षित करना अब केवल बाहरी सुरक्षा को मजबूत करने तक सीमित नहीं है - यह पूरे संस्थान में जुड़े उपकरणों की तेजी से बढ़ती संख्या को प्रबंधित करने के बारे में भी है। MRI स्कैनर और स्मार्ट इन्फ्यूजन पंप से लेकर मरीजों के टैबलेट और आगंतुकों के स्मार्टफोन तक, एंडपॉइंट्स की भारी संख्या और विविधता हमले के लिए एक अभूतपूर्व क्षेत्र बनाती है। नेटवर्क एक्सेस कंट्रोल (NAC) एक महत्वपूर्ण बुनियादी ढांचा है जो नेटवर्क से जुड़ने वाले प्रत्येक उपकरण की पहचान करने, प्रमाणित करने और अधिकृत करने के लिए आवश्यक है, जिससे चिकित्सा उपकरण और मरीजों का डेटा सुरक्षित रहता है।
हेल्थकेयर संगठनों में CTO और IT निदेशकों के लिए, HIPAA, NHS DSP Toolkit और GDPR का अनुपालन करने और जोखिम को प्रभावी ढंग से कम करने के लिए एक मजबूत NAC समाधान तैनात करना बेहद आवश्यक है। हेल्थकेयर परिवेश के लिए तैयार की गई यह मार्गदर्शिका, NAC आर्किटेक्चर, कार्यान्वयन रणनीति और सर्वोत्तम प्रथाओं पर गहराई से नज़र डालती है। हम यह पता लगाएंगे कि शून्य-विश्वास नेटवर्क एक्सेस (zero-trust network access) कैसे प्राप्त किया जाए, नैदानिक IoT उपकरणों को सार्वजनिक ट्रैफ़िक से कैसे अलग किया जाए, और मुख्य नैदानिक नेटवर्क की सुरक्षा से समझौता किए बिना आगंतुक पहुंच को सुरक्षित रूप से प्रबंधित करने के लिए Guest WiFi जैसे समाधानों का उपयोग कैसे किया जाए।
तकनीकी गहराई
हेल्थकेयर नेटवर्क की चुनौती
हेल्थकेयर नेटवर्क विशिष्ट रूप से जटिल होते हैं। उन्हें सख्त अपटाइम और डेटा अखंडता आवश्यकताओं वाले नैदानिक प्रणालियों, पुराने ऑपरेटिंग सिस्टम पर चलने वाले Internet of Medical Things (IoMT) उपकरणों के बड़े बेड़े, कर्मचारियों के खुद के उपकरणों (BYOD), और हजारों अप्रबंधित मरीजों और आगंतुकों के उपकरणों को एक साथ समर्थन देना होता है। पारंपरिक बाहरी सुरक्षा या स्थिर VLAN असाइनमेंट इस माहौल में पूरी तरह से अपर्याप्त है। इसके लिए एक गतिशील, पहचान-संचालित दृष्टिकोण की आवश्यकता होती है, जो पूरे नेटवर्क आर्किटेक्चर में न्यूनतम-विशेषाधिकार पहुंच को लागू करता है।
इस समस्या का पैमाना बहुत बड़ा है। एक सामान्य 500-बिस्तरों वाले अस्पताल में किसी भी समय 10,000 से अधिक जुड़े हुए उपकरण हो सकते हैं। उन उपकरणों में से 30% से भी कम पारंपरिक एंडपॉइंट सुरक्षा एजेंट चलाने में सक्षम होते हैं। शेष 70% (इन्फ्यूजन पंप, मरीज मॉनिटर, इमेजिंग उपकरण, स्मार्ट बेड) को होस्ट-आधारित नियंत्रणों के बजाय नेटवर्क-स्तरीय नियंत्रणों के माध्यम से सुरक्षित किया जाना चाहिए। यह बिल्कुल वही समस्या है जिसे हल करने के लिए NAC को डिज़ाइन किया गया है।
मुख्य NAC आर्किटेक्चर
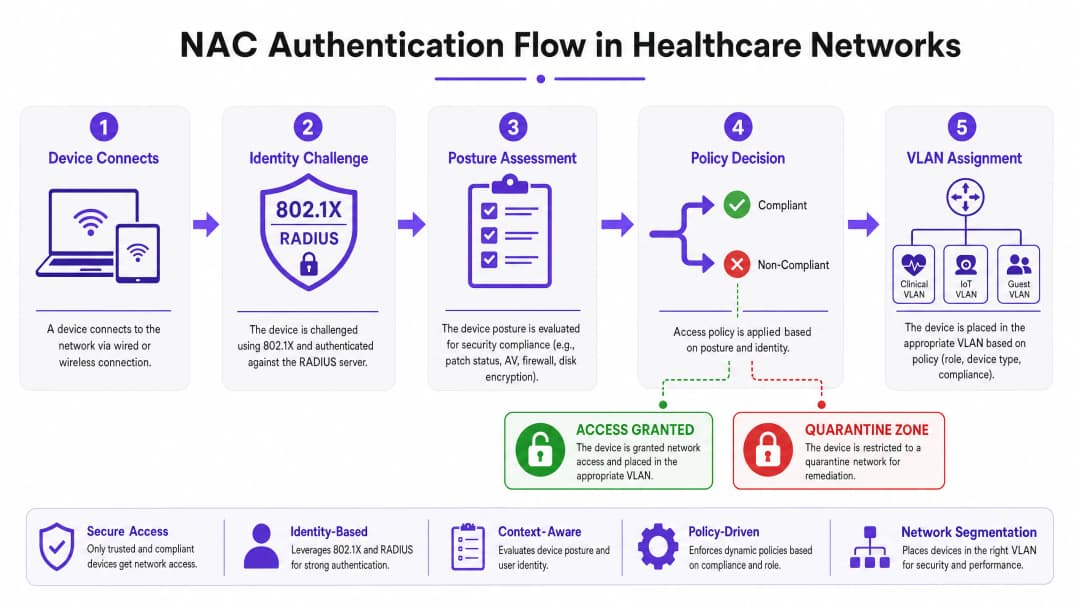
एक हेल्थकेयर परिवेश में प्रोडक्शन-ग्रेड NAC डिप्लॉयमेंट एक साथ काम करने वाले चार मुख्य घटकों पर निर्भर करता है। Supplicant कनेक्टिंग डिवाइस पर क्लाइंट सॉफ़्टवेयर या मूल ऑपरेटिंग सिस्टम घटक है जो ऑथेंटिकेशन एक्सचेंज की शुरुआत करता है। हेडलेस IoT डिवाइस जिनमें supplicant क्षमता नहीं होती है, उनके लिए MAC Authentication Bypass (MAB) का उपयोग फ़ॉलबैक के रूप में किया जाता है। Authenticator नेटवर्क एक्सेस डिवाइस (एक स्विच या वायरलेस एक्सेस पॉइंट) है जो कनेक्शन अनुरोधों को बीच में रोकता है और गेटकीपर के रूप में कार्य करता है, जो ऑथेंटिकेशन सर्वर को क्रेडेंशियल्स फ़ॉरवर्ड करता है। Authentication Server (आमतौर पर एक RADIUS-आधारित पॉलिसी इंजन जैसे Cisco ISE, Aruba ClearPass या ForeScout) सिस्टम का केंद्रीय इंटेलिजेंस है; यह पहचान को सत्यापित करता है, पोस्चर का मूल्यांकन करता है, और डायनेमिक VLAN असाइनमेंट के साथ ऑथराइजेशन निर्णय देता है। अंत में, Directory Store (आमतौर पर Microsoft Active Directory या LDAP) उपयोगकर्ताओं और डिवाइसों के लिए पहचान रिकॉर्ड प्रदान करता है जिनके विरुद्ध RADIUS सर्वर अनुरोधों को सत्यापित करता है।
ऑथेंटिकेशन मैकेनिज्म (Authentication Mechanisms)
पोर्ट-आधारित नेटवर्क एक्सेस कंट्रोल के लिए IEEE 802.1X गोल्ड स्टैंडर्ड है। यह supplicant और ऑथेंटिकेशन सर्वर के बीच EAP (Extensible Authentication Protocol) संदेशों को एनकैप्सुलेट करने के लिए एक ढांचा प्रदान करता है। कॉर्पोरेट-स्वामित्व वाले डिवाइसों के लिए, PEAP-MSCHAPv2 (पासवर्ड-आधारित) के बजाय EAP-TLS (प्रमाणपत्र-आधारित पारस्परिक ऑथेंटिकेशन) की दृढ़ता से अनुशंसा की जाती है। EAP-TLS क्रेडेंशियल चोरी के खतरे को पूरी तरह से समाप्त कर देता है - यदि ऑथेंटिकेशन के लिए आपके आंतरिक PKI द्वारा हस्ताक्षरित एक वैध मशीन प्रमाणपत्र की आवश्यकता होती है, तो केवल एक लीक हुआ पासवर्ड कभी भी नेटवर्क एक्सेस प्रदान नहीं कर सकता है।
MAC Authentication Bypass (MAB) उन डिवाइसों के लिए व्यावहारिक समाधान है जो 802.1X का समर्थन नहीं कर सकते हैं, जिसमें अधिकांश मेडिकल IoT उपकरण शामिल हैं। authenticator डिवाइस के MAC एड्रेस का उपयोग उसकी पहचान क्रेडेंशियल के रूप में करता है। चूंकि MAC एड्रेस को स्पूफ़ किया जा सकता है, इसलिए MAB अपने आप में कमजोर सुरक्षा है, लेकिन गहन डिवाइस प्रोफाइलिंग और व्यावहारिक विश्लेषण के साथ संयुक्त होने पर यह ज्ञात चिकित्सा उपकरणों के प्रबंधन के लिए एक मजबूत नियंत्रण बन जाता है।
मेहमानों और मरीजों की पहुंच के लिए Captive Portal ऑथेंटिकेशन एक तंत्र है। एक अच्छी तरह से लागू किया गया Guest WiFi समाधान उपयोगकर्ता पंजीकरण, सेवा की शर्तों की स्वीकृति और बैंडविड्थ प्रबंधन को संभालता है, जिससे यह सुनिश्चित होता है कि जैसे ही कोई डिवाइस एक्सेस पॉइंट से जुड़ता है, सार्वजनिक ट्रैफ़िक नैदानिक नेटवर्क से पूरी तरह से अलग हो जाता है।
डिवाइस प्रोफाइलिंग और पोस्चर असेसमेंट (Device Profiling and Posture Assessment)
यह जानना कि "कौन" कनेक्ट हो रहा है, केवल आधी लड़ाई है; यह जानना कि वे "किस" डिवाइस के साथ कनेक्ट हो रहे हैं, उतना ही महत्वपूर्ण है। Device Profiling नेटवर्क पर हर डिवाइस को वर्गीकृत करने के लिए पैसिव और एक्टिव नेटवर्क प्रोबिंग तकनीकों (DHCP फिंगरप्रिंट्स, HTTP User-Agent स्ट्रिंग्स, SNMP क्वेरीज़, Nmap-आधारित एक्टिव स्कैनिंग और ट्रैफ़िक पैटर्न विश्लेषण) को जोड़ती है। एक अच्छी तरह से ट्यून किया गया प्रोफाइलिंग इंजन केवल नेटवर्क व्यवहार के आधार पर एक Philips IntelliVue पेशेंट मॉनिटर और Baxter Sigma Spectrum इन्फ्यूजन पंप के बीच अंतर कर सकता है, भले ही दोनों MAB के माध्यम से कनेक्ट होते हों।
Posture Assessment प्रबंधित कॉर्पोरेट डिवाइसेस पर लागू होता है। क्लिनिकल VLAN तक पहुंच प्रदान करने से पहले, NAC सिस्टम अनुपालन के लिए एंडपॉइंट से पूछताछ करता है: क्या ऑपरेटिंग सिस्टम आवश्यक वर्शन में पैच किया गया है? क्या एंटीवायरस सिग्नेचर डेटाबेस अपडेट हैं? क्या फुल-डिस्क एन्क्रिप्शन सक्षम है? जो डिवाइसेस पॉश्चर चेक में विफल रहते हैं, उन्हें डायनामिक रूप से एक रेमेडिएशन VLAN में असाइन किया जाता है जहाँ वे अपडेट प्राप्त कर सकते हैं लेकिन क्लिनिकल सिस्टम तक नहीं पहुँच सकते।
अपने विशिष्ट सेटअप को लेकर कोई सवाल हैं?
हमारी टीम 80,000 से अधिक वेन्यू में वेन्यू ऑपरेटरों, IT मैनेजरों और नेटवर्क इंजीनियरों के साथ काम करती है। 20 मिनट का कॉल बुक करें और हम आपको दिखाएंगे कि आपके जैसे अन्य लोगों ने इसे कैसे हल किया।
Implementation Guide
लाइव अस्पताल के माहौल में NAC को तैनात करने के लिए सावधानीपूर्वक योजना बनाने की आवश्यकता होती है ताकि महत्वपूर्ण देखभाल सेवाओं में कोई बाधा न आए। एक चरणबद्ध दृष्टिकोण की केवल सिफारिश नहीं की जाती है - यह अनिवार्य है।
Phase 1: Discovery and Profiling (Monitor Mode)
मॉनिटर मोड (Monitor Mode) में NAC समाधान को तैनात करके शुरुआत करें। प्रमाणीकरण अनुरोधों को NAC सर्वर पर फॉरवर्ड करने के लिए स्विच और एक्सेस पॉइंट्स को कॉन्फ़िगर करें, लेकिन सर्वर को हर कनेक्शन को लॉग करते हुए सभी एक्सेस की अनुमति देने का निर्देश दें। सभी शिफ्ट पैटर्न और डिवाइस उपयोग चक्रों को कवर करने के लिए इस चरण को कम से कम चार सप्ताह तक चलाएं। इस चरण का आउटपुट नेटवर्क पर प्रत्येक डिवाइस की एक पूर्ण, मान्य इन्वेंट्री है, जिसमें शैडो IT और लीगेसी उपकरण शामिल हैं जो CMDB में दिखाई नहीं दे सकते हैं। डिवाइस प्रोफाइलिंग नियमों को परिष्कृत करने और एन्फोर्समेंट के दौरान विशेष हैंडलिंग की आवश्यकता वाले किसी भी डिवाइस की पहचान करने के लिए इस डेटा का उपयोग करें।
Phase 2: Policy Definition and VLAN Segmentation
डिस्कवरी डेटा के आधार पर, विशिष्ट VLANs पर मैप की गई बारीक एक्सेस नीतियां परिभाषित करें। Clinical VLANs को 802.1X EAP-TLS के माध्यम से प्रमाणित अधिकृत स्टाफ डिवाइसेस और मान्य प्रोफाइलिंग के साथ MAB के माध्यम से प्रमाणित ज्ञात मेडिकल IoT डिवाइसेस तक सीमित होना चाहिए। IoT VLANs को डिवाइस क्लास के आधार पर आगे उप-विभाजित किया जाना चाहिए (उदाहरण के लिए, इन्फ्यूजन पंपों के लिए एक समर्पित VLAN, इमेजिंग उपकरणों के लिए एक अलग VLAN) जिसमें सख्त ACLs केवल विशिष्ट प्रबंधन सर्वरों के साथ संचार की अनुमति देते हैं जिनकी प्रत्येक डिवाइस क्लास को आवश्यकता होती है। Guest VLANs सभी अप्रमाणित ट्रैफ़िक को एक Captive Portal पर निर्देशित करते हैं, जो परिचालन दृश्यता प्रदान करने के लिए एकीकृत WiFi Analytics वाले प्लेटफ़ॉर्म का उपयोग करते हुए आंतरिक नेटवर्क से पूरी तरह से अलग रहता है।
विक्रेता-विशिष्ट कॉन्फ़िगरेशन मार्गदर्शन के लिए, Cisco Meraki में VLAN-स्टीयरिंग NAC नीतियों को कैसे कॉन्फ़िगर करें पर हमारा विस्तृत ट्यूटोरियल देखें।
Phase 3: Gradual Enforcement
Monitor Mode से लागू करने की प्रक्रिया में चरणों में बदलाव करें। Low-Impact Enforcement से शुरुआत करें: बुनियादी ACLs लागू करें जो ज्ञात-खराब ट्रैफ़िक पैटर्न को ब्लॉक करते हैं लेकिन अधिकांश वैध ट्रैफ़िक की अनुमति देते हैं। नैदानिक संचालन को प्रभावित करने से पहले किसी भी नीति गलत कॉन्फ़िगरेशन की पहचान करने और उसे हल करने के लिए इस चरण का उपयोग करें। फिर Closed Mode प्रवर्तन में संक्रमण करें, जिसे विभाग दर विभाग शुरू किया जाए - पहले प्रशासनिक क्षेत्र, फिर नैदानिक सहायता क्षेत्र, और अंत में गंभीर देखभाल इकाइयाँ। प्रत्येक चरण में, एक त्वरित रोलबैक प्रक्रिया बनाए रखें और सुनिश्चित करें कि प्रवर्तन के बाद चिकित्सा उपकरण सही ढंग से कार्य कर रहे हैं, इसकी पुष्टि करने के लिए क्लीनिकल इंजीनियरिंग टीमें स्टैंडबाय पर हों।
सर्वश्रेष्ठ अभ्यास (Best Practices)
प्रमाणपत्र-आधारित प्रमाणीकरण लागू करें। सभी कॉर्पोरेट-स्वामित्व वाले उपकरणों के लिए, आंतरिक PKI द्वारा जारी मशीन प्रमाणपत्रों के साथ EAP-TLS ही एकमात्र स्वीकृत प्रमाणीकरण विधि होनी चाहिए। पासवर्ड एक दायित्व हैं; प्रमाणपत्र नहीं।
मेडिकल IoT का सूक्ष्म-विभाजन (Micro-segment) करें। सभी चिकित्सा उपकरणों को एक ही IoT VLAN में न डालें। डिवाइस वर्ग द्वारा विभाजित करें और ज़ीरो-ट्रस्ट ACLs लागू करें। एक इन्फ्यूजन पंप को अपने विशिष्ट प्रबंधन सर्वर और EMR सिस्टम तक पहुँचने में सक्षम होना चाहिए - और कुछ नहीं। डिवाइस वर्गों के बीच पार्श्व गतिविधि को नेटवर्क लेयर पर ब्लॉक किया जाना चाहिए।
निरंतर व्यवहार संबंधी निगरानी लागू करें। NAC एक बार सेट करके भूल जाने वाला नियंत्रण नहीं है। अपने NAC पॉलिसी इंजन को SIEM या नेटवर्क डिटेक्शन एंड रिस्पांस (NDR) प्लेटफॉर्म के साथ एकीकृत करें। यदि प्रोफाइल किया गया IoT डिवाइस असामान्य व्यवहार प्रदर्शित करना शुरू करता है - जैसे अप्रत्याशित पोर्ट स्कैनिंग, असामान्य आउटबाउंड कनेक्शन - तो NAC सिस्टम को मानवीय हस्तक्षेप की प्रतीक्षा किए बिना इसे गतिशील रूप से क्वारंटाइन करना चाहिए।
अपने वायरलेस बुनियादी ढांचे को अनुकूलित करें। सुनिश्चित करें कि आपका एक्सेस पॉइंट परिनियोजन प्रत्येक नैदानिक क्षेत्र में डिवाइस घनत्व के लिए पर्याप्त कवरेज और क्षमता प्रदान करता है। विभिन्न वायरलेस बैंड के प्रभावों को समझना आवश्यक है - हमारा गाइड Wi Fi Frequencies: A Guide to Wi-Fi Frequencies in 2026 मिश्रित IoT और नैदानिक वातावरण में 2.4 GHz, 5 GHz और 6 GHz के बीच व्यावहारिक समझौतों को कवर करता है।
अतिथि पहुंच को एक प्रथम श्रेणी सुरक्षा नियंत्रण के रूप में एकीकृत करें। गेस्ट WiFi कोई वैकल्पिक अतिरिक्त सुविधा नहीं है - यह आपके नेटवर्क पर सबसे अधिक जोखिम वाले ट्रैफ़िक प्रकारों में से एक है। एक समर्पित Guest WiFi प्लेटफॉर्म यह सुनिश्चित करता है कि रोगी और आगंतुक उपकरण नैदानिक नेटवर्क से अलग हों, स्वतंत्र रूप से प्रमाणित और प्रबंधित हों। इसके परिणामस्वरूप मिलने वाला WiFi Analytics डेटा रोगी प्रवाह और सुविधा प्रबंधन में परिचालन सुधारों का भी समर्थन करता है।
समस्या निवारण और जोखिम न्यूनीकरण
सामान्य विफलता मोड
Silent IoT Device हेल्थकेयर NAC डिप्लॉयमेंट में सबसे आम परिचालन समस्या है। एक मेडिकल डिवाइस जो कम-पावर स्लीप स्टेट में चली जाती है, वह अपना नेटवर्क कनेक्शन खो देती है और जागने पर फिर से सही ढंग से री-ऑथेंटिकेट करने में विफल रहती है। इसका परिणाम यह होता है कि डिवाइस NAC सिस्टम में ऑफलाइन दिखाई देता है लेकिन शारीरिक रूप से मौजूद होता है और काम करने का प्रयास कर रहा होता है। इसके समाधानों में प्रत्येक डिवाइस श्रेणी के अपेक्षित स्लीप साइकिल से मेल खाने के लिए स्विच पर MAC एजिंग टाइमर को ट्यून करना और पूर्ण री-ऑथेंटिकेशन साइकिल की आवश्यकता के बिना वापस आने वाले डिवाइस को पहचानने के लिए NAC प्रोफाइलिंग इंजन को कॉन्फ़िगर करना शामिल है।
यदि सक्रिय रूप से प्रबंधित नहीं किया गया, तो सर्टिफिकेट की समय सीमा समाप्त होना (Certificate expiry) एक प्रणालीगत जोखिम है जो एक साथ सैकड़ों स्टाफ उपकरणों को लॉक आउट कर सकता है। SCEP या EST प्रोटोकॉल का उपयोग करके स्वचालित सर्टिफिकेट लाइफसाइकिल मैनेजमेंट लागू करें और 60 दिनों के भीतर समाप्त होने वाले सर्टिफिकेट के लिए अलर्ट कॉन्फ़िगर करें। सामूहिक रूप से एक साथ समाप्त होने से बचने के लिए डिवाइस समूहों में सर्टिफिकेट रिन्यूअल साइकिल को चरणबद्ध करें।
RADIUS सर्वर मिसकॉन्फ़िगरेशन - नेटवर्क एक्सेस डिवाइस पर गलत IP एड्रेस, बेमेल शेयर्ड सीक्रेट या मिसकॉन्फ़िगर किए गए EAP तरीके - साइलेंट ऑथेंटिकेशन विफलताओं का कारण बनते हैं जिन्हें उचित लॉगिंग के बिना डायग्नोस करना कठिन होता है। सभी स्विच और एक्सेस पॉइंट्स पर मानकीकृत RADIUS कॉन्फ़िगरेशन को पुश करने के लिए सेंट्रलाइज्ड नेटवर्क मैनेजमेंट का उपयोग करें और सभी ऑथेंटिकेशन इवेंट्स का ऑडिट ट्रेल प्रदान करने के लिए RADIUS अकाउंटिंग लागू करें।
फेल-ओपन बनाम फेल-क्लोज्ड निर्णय
हेल्थकेयर NAC डिप्लॉयमेंट में यह सबसे महत्वपूर्ण आर्किटेक्चरल निर्णय है। एक फेल-क्लोज्ड पॉलिसी (यदि NAC सर्वर तक नहीं पहुंचा जा सकता है तो नेटवर्क एक्सेस को अस्वीकार करें) सबसे मजबूत सुरक्षा प्रदान करती है लेकिन सर्वर आउटेज के दौरान जीवन-महत्वपूर्ण मेडिकल डिवाइस को अलग-थलग करने का जोखिम उठाती है। एक फेल-ओपन पॉलिसी (यदि सर्वर विफल हो जाता है तो सीमित पहुंच प्रदान करें) नैदानिक निरंतरता बनाए रखती है लेकिन कम सुरक्षा नियंत्रण की अवधि बनाती है। अनुशंसित दृष्टिकोण एक टियर फेल्योर पॉलिसी है: मजबूत नेटवर्क-लेवल ACLs द्वारा समर्थित महत्वपूर्ण नैदानिक VLANs के लिए फेल-ओपन, जबकि प्रशासनिक और गेस्ट VLANs फेल-क्लोज्ड होते हैं। इस निर्णय की आवश्यकता को कम करने के लिए कई भौतिक स्थानों या उपलब्धता क्षेत्रों में हाई-अवेलेबिलिटी क्लस्टर में NAC पॉलिसी इंजन तैनात करें।
ROI और व्यावसायिक प्रभाव
हेल्थकेयर में NAC को तैनात करने का बिजनेस केस कई आयामों में आकर्षक है। प्राथमिक चालक जोखिम में कमी है: रेगुलेटरी जुर्माने, कानूनी लागतों, समाधान खर्चों और प्रतिष्ठा को होने वाले नुकसान को शामिल करने के बाद प्रोटेक्टेड हेल्थ इंफॉर्मेशन (PHI) से जुड़े एक सिंगल रिपोर्ट करने योग्य डेटा ब्रीच की औसत लागत $10 मिलियन से अधिक हो जाती है। NAC सीधे तौर पर ऐसी घटना की संभावना और संभावित प्रभाव क्षेत्र दोनों को कम करता है, यह सुनिश्चित करके कि केवल अधिकृत, अनुपालन करने वाले डिवाइस ही PHI वाले सिस्टम तक पहुंच सकें।परिचालन दक्षता (Operational efficiency) एक द्वितीयक लेकिन महत्वपूर्ण लाभ है। स्वचालित डिवाइस प्रोफाइलिंग और ऑनबोर्डिंग उस मैन्युअल स्विच-पोर्ट कॉन्फ़िगरेशन को समाप्त करती है जो NAC के बिना वाले वातावरणों में IT सर्विस डेस्क का काफी समय लेती है। क्लीनिकल इंजीनियरिंग टीमों को लाइफसाइकिल मैनेजमेंट, रखरखाव शेड्यूलिंग और खरीद योजना का समर्थन करने के लिए रीयल-टाइम, सटीक डिवाइस इन्वेंट्री मिलती है।
अनुपालन स्थिति (Compliance posture) में सीधे सुधार होता है। HIPAA का एक्सेस कंट्रोल मानक (45 CFR §164.312(a)(1)), NHS DSP Toolkit की साइबर सुरक्षा आवश्यकताएं, और GDPR Article 32 के प्रोसेसिंग-की-सुरक्षा संबंधी दायित्व, सभी इस बात पर स्पष्ट नियंत्रण की मांग करते हैं कि कौन से लोग और डिवाइस मरीज के डेटा वाले सिस्टम तक पहुंच सकते हैं। एक अच्छी तरह से प्रलेखित NAC परिनियोजन इन दायित्वों को पूरा करने के लिए आवश्यक ऑडिट साक्ष्य प्रदान करता है।
अंततः, एक अच्छी तरह से लागू की गई अतिथि एक्सेस रणनीति से मरीज के अनुभव (patient experience) को लाभ होता है। मरीजों और आगंतुकों के लिए विश्वसनीय, सुरक्षित Guest WiFi संतुष्टि स्कोर में सुधार करता है, जबकि अंतर्निहित WiFi Analytics डेटा बेड प्रबंधन, विज़िटर फ्लो और सुविधाओं के उपयोग में परिचालन संबंधी सुधारों का समर्थन करता है।
मुख्य परिभाषाएं
Network Access Control (NAC)
एक सुरक्षा ढांचा जो नीति-आधारित नियंत्रण लागू करता है कि किन उपकरणों और उपयोगकर्ताओं को नेटवर्क से जुड़ने की अनुमति है, और कनेक्ट होने के बाद वे किन संसाधनों तक पहुंच सकते हैं। NAC प्रमाणीकरण, डिवाइस प्रोफाइलिंग, पोस्चर मूल्यांकन और गतिशील नीति प्रवर्तन को जोड़ता है।
IT टीमें NAC को एक उत्पाद श्रेणी (Cisco ISE, Aruba ClearPass, ForeScout) और एक आर्किटेक्चरल दृष्टिकोण दोनों के रूप में देखती हैं। स्वास्थ्य सेवा में, क्लीनिकल सिस्टम, मेडिकल IoT और अतिथि WiFi पहुंच के बीच नेटवर्क पृथक्करण को लागू करने के लिए NAC प्राथमिक तंत्र है।
IEEE 802.1X
पोर्ट-आधारित नेटवर्क एक्सेस कंट्रोल के लिए एक IEEE मानक जो LAN या WLAN से जुड़ने के इच्छुक उपकरणों के लिए एक प्रमाणीकरण ढांचा प्रदान करता है। यह सप्लिकेंट (क्लाइंट), ऑथेंटिकेटर (स्विच/AP) और प्रमाणीकरण सर्वर (RADIUS) की भूमिकाओं को परिभाषित करता है, और उनके बीच EAP संदेशों को समाहित करता है।
NAC परिनियोजन में कॉर्पोरेट-स्वामित्व वाले उपकरणों के लिए 802.1X प्रमाणीकरण तंत्र है। IT टीमें इसे नेटवर्क एक्सेस डिवाइस (स्विच, AP) और एंडपॉइंट डिवाइस (OS-स्तर की सप्लिकेंट सेटिंग्स या Group Policy के माध्यम से) दोनों पर कॉन्फ़िगर करती हैं।
MAC Authentication Bypass (MAB)
उन उपकरणों के लिए उपयोग किया जाने वाला एक वैकल्पिक प्रमाणीकरण तंत्र जो 802.1X का समर्थन नहीं कर सकते हैं। नेटवर्क एक्सेस डिवाइस कनेक्ट करने वाले उपकरण के MAC एड्रेस को उसकी पहचान क्रेडेंशियल के रूप में उपयोग करता है, और इसे प्राधिकरण के लिए RADIUS सर्वर पर भेजता है।
स्वास्थ्य सेवा NAC परिनियोजन में मेडिकल IoT उपकरणों के लिए MAB प्राथमिक प्रमाणीकरण विधि है। सार्थक सुरक्षा प्रदान करने के लिए इसे डिवाइस प्रोफाइलिंग के साथ जोड़ा जाना चाहिए, क्योंकि MAC एड्रेस को स्पूफ़ किया जा सकता है।
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
एक प्रमाणपत्र-आधारित EAP विधि जो X.509 डिजिटल प्रमाणपत्रों का उपयोग करके क्लाइंट और प्रमाणीकरण सर्वर के बीच पारस्परिक प्रमाणीकरण प्रदान करती है। क्लाइंट और सर्वर दोनों प्रमाणपत्र प्रस्तुत करते हैं, जिससे पासवर्ड-आधारित क्रेडेंशियल चोरी का खतरा समाप्त हो जाता है।
स्वास्थ्य सेवा NAC परिनियोजन में कॉर्पोरेट उपकरणों के लिए EAP-TLS अनुशंसित प्रमाणीकरण विधि है। इसके लिए मशीन प्रमाणपत्र जारी करने और प्रबंधित करने के लिए एक कार्यशील आंतरिक PKI की आवश्यकता होती है।
VLAN Steering
NAC सिस्टम से ऑथेंटिकेशन परिणाम और नीति निर्णय के आधार पर एक कनेक्टिंग डिवाइस का एक विशिष्ट VLAN को डायनेमिक असाइनमेंट। RADIUS सर्वर Access-Accept प्रतिक्रिया के भाग के रूप में एक VLAN ID (या VLAN नाम) लौटाता है, और ऑथेंटिकेटर डिवाइस के पोर्ट को उस VLAN में रखता है।
VLAN स्टीयरिंग वह तंत्र है जिसके द्वारा NAC नेटवर्क सेगमेंटेशन लागू करता है। IT टीमें प्रत्येक डिवाइस श्रेणी के लिए लक्षित VLAN निर्दिष्ट करने के लिए ऑथेंटिकेशन सर्वर पर RADIUS विशेषताएँ (Tunnel-Type, Tunnel-Medium-Type, Tunnel-Private-Group-ID) कॉन्फ़िगर करती हैं।
डिवाइस प्रोफाइलिंग (Device Profiling)
पैसिव नेटवर्क प्रोब्स (DHCP फिंगरप्रिंट, HTTP User-Agent स्ट्रिंग्स, mDNS/Bonjour विज्ञापन) और एक्टिव स्कैनिंग तकनीकों (Nmap, SNMP क्वेरी) का उपयोग करके कनेक्टिंग डिवाइस के प्रकार, निर्माता और ऑपरेटिंग सिस्टम की पहचान करने की प्रक्रिया।
स्वास्थ्य सेवा NAC परिनियोजन में मेडिकल IoT उपकरणों को सटीक रूप से वर्गीकृत करने के लिए डिवाइस प्रोफाइलिंग आवश्यक है। प्रोफाइलिंग के बिना, MAB-ऑथेंटिकेटेड डिवाइस एक-दूसरे से अप्रभेद्य होते हैं, जिससे डिवाइस-वर्ग-विशिष्ट एक्सेस नीतियां लागू करना असंभव हो जाता है।
पोस्चर असेसमेंट (Posture Assessment)
नेटवर्क एक्सेस देने से पहले कनेक्टिंग डिवाइस की सुरक्षा अनुपालन स्थिति का मूल्यांकन। पोस्चर चेक आमतौर पर OS पैच स्तर, एंटीवायरस सिग्नेचर करेंसी, डिस्क एन्क्रिप्शन स्थिति और आवश्यक सुरक्षा सॉफ़्टवेयर की उपस्थिति की पुष्टि करते हैं।
पोस्चर असेसमेंट स्वास्थ्य सेवा NAC परिनियोजन में प्रबंधित कॉर्पोरेट उपकरणों (लैपटॉप, वर्कस्टेशन) पर लागू होता है। जो डिवाइस पोस्चर चेक में विफल रहते हैं, उन्हें डायनेमिक रूप से एक रेमेडिएशन VLAN में असाइन किया जाता है जहां वे अपडेट प्राप्त कर सकते हैं लेकिन नैदानिक प्रणालियों तक नहीं पहुंच सकते हैं।
क्वारंटाइन VLAN (Quarantine VLAN)
एक प्रतिबंधित नेटवर्क सेगमेंट जिसमें गैर-अनुपालन या अपरिचित उपकरणों को तब असाइन किया जाता है जब वे ऑथेंटिकेशन या पोस्चर असेसमेंट में विफल हो जाते हैं। क्वारंटाइन VLAN आम तौर पर केवल रेमेडिएशन संसाधनों (पैच सर्वर, एंटीवायरस अपडेट सर्वर) तक पहुंच प्रदान करता है और सभी नैदानिक और कॉर्पोरेट प्रणालियों तक पहुंच को अवरुद्ध करता है।
IT टीमें NAC नीति उल्लंघनों के लिए प्रवर्तन तंत्र के रूप में क्वारंटाइन VLANs का उपयोग करती हैं। क्वारंटाइन VLAN में एक डिवाइस प्रभावी रूप से शेष नेटवर्क से अलग हो जाता है, जबकि अनुपालन प्राप्त करने के लिए आवश्यक अपडेट प्राप्त करने में सक्षम रहता है।
IoMT (इंटरनेट ऑफ मेडिकल थिंग्स)
कनेक्टेड मेडिकल उपकरणों और स्वास्थ्य सेवा अनुप्रयोगों का पारिस्थितिकी तंत्र जो रोगी डेटा एकत्र करने और प्रसारित करने के लिए नेटवर्क पर संचार करते हैं। IoMT में इन्फ्यूजन पंप, रोगी मॉनिटर, इमेजिंग उपकरण, स्मार्ट बेड और पहनने योग्य स्वास्थ्य मॉनिटर शामिल हैं।
IoMT डिवाइस स्वास्थ्य सेवा NAC परिनियोजन में सबसे बड़ी और सबसे चुनौतीपूर्ण डिवाइस श्रेणी का प्रतिनिधित्व करते हैं। वे आम तौर पर विरासत ऑपरेटिंग सिस्टम चलाते हैं, एंडपॉइंट सुरक्षा एजेंटों का समर्थन नहीं कर सकते हैं, और उन्हें विशेष प्रोफाइलिंग और माइक्रो-सेगमेंटेशन रणनीतियों की आवश्यकता होती है।
Zero-Trust Network Access (ZTNA)
एक सुरक्षा मॉडल जो नेटवर्क आर्किटेक्चर से अंतर्निहित विश्वास को समाप्त करता है। ZTNA के तहत, किसी भी डिवाइस या उपयोगकर्ता पर उनके नेटवर्क स्थान की परवाह किए बिना डिफ़ॉल्ट रूप से भरोसा नहीं किया जाता है। प्रत्येक एक्सेस अनुरोध को स्पष्ट रूप से ऑथेंटिकेट, अधिकृत और लगातार सत्यापित किया जाना चाहिए।
ZTNA वह आर्किटेक्चरल दर्शन है जो आधुनिक NAC परिनियोजन को रेखांकित करता है। स्वास्थ्य सेवा में, ZTNA का अर्थ है कि क्लिनिकल VLAN पर मौजूद डिवाइस को भी लगातार अपनी पहचान और अनुपालन स्थिति साबित करनी होगी - केवल नेटवर्क स्थान संवेदनशील प्रणालियों तक पहुंच प्रदान नहीं करता है।
हल किए गए उदाहरण
एक 350-बेड वाला NHS Trust अपने वार्षिक DSP Toolkit सबमिशन के लिए तैयारी कर रहा है। IT निदेशक ने पहचान की है कि नेटवर्क में वर्तमान में कोई डिवाइस ऑथेंटिकेशन नहीं है - सब कुछ एक सिंगल VLAN वाले फ्लैट नेटवर्क से जुड़ता है। लगभग 2,400 कनेक्टेड डिवाइस हैं, जिनमें से अनुमानित 800 मेडिकल IoT डिवाइस (इन्फ्यूजन पंप, रोगी मॉनिटर, वेंटिलेटर) हैं। Trust को क्लिनिकल ऑपरेशन्स को बाधित किए बिना 6 महीने के भीतर अनुपालन प्राप्त करने की आवश्यकता है। वे कहाँ से शुरू करें?
यह कार्य 4-सप्ताह के मॉनिटर मोड डिप्लॉयमेंट के साथ शुरू होता है। सभी कोर स्विच और वायरलेस कंट्रोलर को 802.1X और MAB अनुरोधों को नए तैनात RADIUS पॉलिसी इंजन (Cisco ISE या Aruba ClearPass इस स्केल के लिए अग्रणी विकल्प हैं) पर अग्रेषित करने के लिए कॉन्फ़िगर करें। सर्वर को परमिट-ऑल लेकिन लॉग-एवरीथिंग पर सेट किया गया है। 4 सप्ताह के बाद, सभी 2,400 उपकरणों को वर्गीकृत करने के लिए प्रोफाइलिंग डेटा का विश्लेषण करें। लगभग 800 मेडिकल IoT डिवाइस (MAB उम्मीदवार), 600 कॉर्पोरेट वर्कस्टेशन और लैपटॉप (802.1X उम्मीदवार), 400 स्टाफ BYOD डिवाइस और 600 रोगी/विज़िटर डिवाइस मिलने की उम्मीद है। सप्ताह 5-8 में, VLAN आर्किटेक्चर को परिभाषित करें: स्टाफ उपकरणों और EMR-कनेक्टेड सिस्टम के लिए क्लिनिकल VLAN (10.10.0.0/22), विशिष्ट प्रबंधन सर्वरों तक संचार को प्रतिबंधित करने वाले ACLs के साथ मेडिकल उपकरणों के लिए IoT VLAN (10.20.0.0/22), और एक Captive Portal पर रूट किया गया गेस्ट VLAN (10.30.0.0/22)। रोगी-सामना वाले नेटवर्क के लिए एक समर्पित गेस्ट WiFi प्लेटफॉर्म तैनात करें। सप्ताह 9-16 में, प्रशासनिक ब्लॉक से शुरू करते हुए श्रेणीबद्ध प्रवर्तन शुरू करें। सप्ताह 17-24 में, प्रवर्तन से पहले क्लिनिकल इंजीनियरिंग के साथ प्रत्येक मेडिकल डिवाइस क्लास को मान्य करते हुए, क्लिनिकल क्षेत्रों में प्रवर्तन का विस्तार करें। छठे महीने तक, Trust के पास प्रलेखित एक्सेस कंट्रोल के साथ पूरी तरह से विभाजित नेटवर्क होता है, जो DSP Toolkit आवश्यकता 5 (एक्सेस कंट्रोल) को संतुष्ट करता है और सबमिशन के लिए आवश्यक ऑडिट साक्ष्य प्रदान करता है।
एक निजी अस्पताल समूह एक नए ऑन्कोलॉजी विंग का समर्थन करने के लिए अपने नेटवर्क का विस्तार कर रहा है जिसमें 150 नए कनेक्टेड मेडिकल डिवाइस शामिल हैं, जिसमें दो अलग-अलग निर्माताओं के 40 इन्फ्यूजन पंप, 60 रोगी मॉनिटर और 50 मिश्रित डिवाइस (स्मार्ट बेड, नर्स कॉल सिस्टम) शामिल हैं। नेटवर्क टीम के पास एक मौजूदा Cisco Meraki इन्फ्रास्ट्रक्चर है जिसमें कोई NAC नहीं है। CISO चाहता है कि 8 सप्ताह में विंग खुलने से पहले माइक्रो-सेगमेंटेशन लागू हो जाए। डिप्लॉयमेंट रणनीति क्या है?
मौजूदा इन्फ्रास्ट्रक्चर के रूप में Cisco Meraki के साथ, यह परिनियोजन Meraki के इन-बिल्ट RADIUS एकीकरण और Group Policy सुविधाओं का लाभ उठाता है। सबसे पहले, एक RADIUS सर्वर (FreeRADIUS या Cisco ISE) परिनियोजित करें और नए विंग के सभी Meraki स्विच और MR एक्सेस पॉइंट्स को प्रमाणीकरण के लिए इसका उपयोग करने के लिए कॉन्फ़िगर करें। सभी मेडिकल उपकरणों के लिए MAB कॉन्फ़िगर करें, उपकरण वर्गीकरण में सहायता के लिए Meraki के क्लाइंट फ़िंगरप्रिंटिंग का उपयोग करें। Meraki डैशबोर्ड में तीन Group Policies परिभाषित करें: IoT-InfusionPumps (VLAN 210, ACL जो केवल 10.10.5.20 पर इन्फ्यूजन पंप प्रबंधन सर्वर और 10.10.1.10 पर EMR के ट्रैफ़िक की अनुमति देता है), IoT-PatientMonitors (VLAN 220, ACL जो 10.10.5.30 पर मॉनिटरिंग सर्वर और EMR के ट्रैफ़िक की अनुमति देता है), और IoT-General (VLAN 230, मिश्रित उपकरणों के लिए अधिक उदार ACL)। खरीद दस्तावेज़ों से प्राप्त सभी 150 उपकरणों के MAC एड्रेस को RADIUS सर्वर में पहले से दर्ज (Pre-populate) करें। विंग के सॉफ्ट ओपनिंग के पहले दो हफ्तों के लिए इसे मॉनिटर मोड में चलाएं, यह सत्यापित करते हुए कि सभी उपकरण सही ढंग से प्रोफाइल और असाइन किए गए हैं। सप्ताह 3 में पूर्ण प्रवर्तन (full enforcement) पर जाएं। विस्तृत Meraki-विशिष्ट VLAN स्टीयरिंग कॉन्फ़िगरेशन के लिए, इस गाइड को देखें How to Configure NAC Policies for VLAN Steering in Cisco Meraki ।
अभ्यास प्रश्न
Q1. एक क्षेत्रीय अस्पताल में 1,200 कनेक्टेड डिवाइस हैं। मॉनिटर मोड NAC परिनियोजन के दौरान, प्रोफाइलिंग इंजन अज्ञात प्रोफाइल वाले 340 उपकरणों की पहचान करता है - वे किसी भी ज्ञात मेडिकल डिवाइस फिंगरप्रिंट से मेल नहीं खा रहे हैं और कॉर्पोरेट वर्कस्टेशन भी नहीं हैं। CISO 2 सप्ताह में प्रवर्तन पर जाना चाहता है। कार्रवाई का सही तरीका क्या है, और CISO की समयसीमा पर आगे बढ़ने के क्या जोखिम हैं?
संकेत: विचार करें कि वे 340 अज्ञात डिवाइस क्या हो सकते हैं, और यदि वे अवर्गीकृत रहते हैं तो प्रवर्तन लाइव होने पर उनका क्या होगा।
मॉडल उत्तर देखें
सही कार्रवाई प्रवर्तन में तब तक देरी करना है जब तक कि 340 अज्ञात उपकरणों की जांच और वर्गीकरण नहीं हो जाता। प्रवर्तन लाइव होने पर इन उपकरणों को क्वारंटाइन VLAN में रखा जाएगा, जिसमें ऐसे चिकित्सा उपकरण भी शामिल हो सकते हैं जो रोगी की देखभाल के लिए अत्यंत महत्वपूर्ण हैं। जांच में शामिल होना चाहिए: (1) संभावित उपकरण प्रकारों की पहचान करने के लिए निर्माता डेटाबेस के खिलाफ MAC address OUI उपसर्गों को क्रॉस-रेफरेंस करना, (2) भौतिक रूप से उपकरणों की पहचान करने के लिए स्विच पोर्ट स्थानों की समीक्षा करना, (3) CMDB में नहीं मौजूद किसी भी चिकित्सा उपकरण की पहचान करने के लिए क्लिनिकल इंजीनियरिंग को शामिल करना, और (4) होस्टनाम पैटर्न के लिए DHCP लॉग की समीक्षा करना। सभी 340 उपकरणों को वर्गीकृत करने और उचित नीतियां परिभाषित होने के बाद ही प्रवर्तन आगे बढ़ना चाहिए। CISO की 2-सप्ताह की समयसीमा पर आगे बढ़ने का जोखिम एक संभावित रोगी सुरक्षा घटना है यदि किसी आपातकालीन देखभाल परिदृश्य के दौरान एक अवर्गीकृत चिकित्सा उपकरण को क्वारंटाइन किया जाता है।
Q2. एक IT आर्किटेक्ट एक नए अस्पताल विंग के लिए NAC विफलता मोड नीति डिजाइन कर रहा है। क्लिनिकल डायरेक्टर का आग्रह है कि चिकित्सा उपकरणों का नेटवर्क कनेक्शन कभी नहीं छूटना चाहिए, भले ही NAC सर्वर ऑफलाइन हो जाए। CISO सभी VLAN के लिए फेल-क्लोज्ड पर जोर देता है। आप इस संघर्ष को कैसे हल करेंगे, और किन क्षतिपूर्ति नियंत्रणों की आवश्यकता है?
संकेत: टियर विफलता नीतियों के बारे में सोचें और आउटेज के दौरान NAC नीति प्रवर्तन के विकल्प के रूप में कौन से नेटवर्क-स्तरीय नियंत्रण काम कर सकते हैं।
मॉडल उत्तर देखें
इसका समाधान एक टियर विफलता नीति है जो दोनों आवश्यकताओं को पूरा करती है। IoT VLAN और क्लिनिकल VLAN को फेल-ओपन (यदि RADIUS सर्वर पहुंच योग्य नहीं है तो पहुंच की अनुमति दें) के लिए कॉन्फ़िगर किया गया है, जबकि गेस्ट VLAN और प्रशासनिक VLAN को फेल-क्लोज्ड के लिए कॉन्फ़िगर किया गया है। क्षतिपूर्ति नियंत्रण जो क्लिनिकल VLAN के लिए फेल-ओपन नीति को स्वीकार्य बनाते हैं, वे हैं: (1) VLAN गेटवे पर लागू सख्त ACL जो NAC स्थिति की परवाह किए बिना इंटर-VLAN ट्रैफ़िक को प्रतिबंधित करते हैं, (2) विफलता मोड के ट्रिगर होने की संभावना को कम करने के लिए NAC सर्वर हाई अवेलेबिलिटी डिप्लॉयमेंट (दो डेटा केंद्रों में एक्टिव-एक्टिव क्लस्टर), (3) NAC आउटेज के दौरान असामान्य ट्रैफ़िक का पता लगाने के लिए क्लिनिकल VLAN पर नेटवर्क-स्तरीय IDS/IPS मॉनिटरिंग, और (4) NAC आउटेज परिदृश्यों के लिए प्रलेखित घटना प्रतिक्रिया प्रक्रियाएं। यह दृष्टिकोण क्लिनिकल डायरेक्टर की उपलब्धता की आवश्यकता को पूरा करता है और CISO को प्रलेखित क्षतिपूर्ति नियंत्रण प्रदान करता है जो एक स्वीकार्य सुरक्षा स्थिति बनाए रखते हैं।
Q3. एक अस्पताल का NAC डिप्लॉयमेंट 3 महीने से पूर्ण प्रवर्तन मोड में चल रहा है। सुरक्षा टीम को एक अलर्ट प्राप्त होता है कि IoT VLAN पर एक उपकरण (एक इन्फ्यूजन पंप के रूप में प्रोफाइल किया गया) पोर्ट 443 पर एक बाहरी IP पते पर आउटबाउंड कनेक्शन स्थापित करने का प्रयास कर रहा है। उपकरण का MAC address अपेक्षित प्रोफ़ाइल से मेल खाता है। तत्काल प्रतिक्रिया क्या है, और यह घटना NAC आर्किटेक्चर के बारे में क्या संकेत देती है?
संकेत: तात्कालिक नियंत्रण कार्रवाई और उस आर्किटेक्चरल कमी दोनों पर विचार करें जिसने इस ट्रैफ़िक के प्रयास की अनुमति दी (भले ही इसे ब्लॉक कर दिया गया हो)।
मॉडल उत्तर देखें
तत्काल प्रतिक्रिया NAC नीति इंजन के माध्यम से उपकरण को गतिशील रूप से क्वारंटाइन करना है, जांच लंबित रहने तक इसे IoT VLAN से अलग करना है। सुरक्षा टीम को ट्रैफ़िक सामग्री का विश्लेषण करने के लिए उपकरण के स्विच पोर्ट से पैकेट ट्रेस कैप्चर करना चाहिए, और क्लिनिकल इंजीनियरिंग को भौतिक रूप से उपकरण का निरीक्षण करने और यदि आवश्यक हो तो इसे ऑफलाइन करने के लिए अधिसूचित किया जाना चाहिए। यह घटना दो आर्किटेक्चरल मुद्दों को इंगित करती है: (1) IoT VLAN पर ACL इन्फ्यूजन पंपों से आउटबाउंड इंटरनेट ट्रैफ़िक को ब्लॉक नहीं कर रहा है - ACL को केवल विशिष्ट प्रबंधन सर्वर IP और EMR के ट्रैफ़िक की अनुमति देनी चाहिए, जिसमें अन्य सभी गंतव्यों के लिए एक स्पष्ट डेनाइ-ऑल (deny-all) नियम हो; और (2) व्यवहार संबंधी निगरानी एकीकरण ठीक से काम कर रहा है (अलर्ट उत्पन्न हुआ था), लेकिन ACL को ट्रैफ़िक के प्रयास से पहले ही उसे ब्लॉक कर देना चाहिए था। सुधारात्मक कार्रवाई प्रत्येक उपकरण वर्ग के लिए केवल स्पष्ट रूप से आवश्यक संचार पथों की अनुमति देकर, डिफ़ॉल्ट-डेनाइ (default-deny) नीति लागू करने के लिए IoT VLAN ACL को कड़ा करना है।
इस श्रृंखला में आगे पढ़ें
PPSK WPA3: सुविधाओं और परिनियोजन मॉडलों की तुलना
यह तकनीकी संदर्भ गाइड PPSK और WPA3-SAE की तुलना करती है, मल्टी-टेनेंट वातावरण के लिए उनके आर्किटेक्चरल अंतर और परिनियोजन मॉडल की व्याख्या करती है। यह IT प्रबंधकों और प्रॉपर्टी डेवलपर्स को Purple के पहचान-आधारित समाधानों का उपयोग करके सुरक्षित, पृथक WiFi नेटवर्क प्राप्त करने पर व्यावहारिक मार्गदर्शन प्रदान करती है.
PPSK WiFi: विशेषताओं और परिनियोजन (deployment) मॉडलों की तुलना
यह तकनीकी संदर्भ मार्गदर्शिका पारंपरिक 802.1X और मानक PSK परिनियोजनों के मुकाबले Private Pre-Shared Key (PPSK) WiFi आर्किटेक्चर की तुलना करती है। यह नेटवर्क आर्किटेक्ट्स और IT प्रबंधकों को मल्टी-टेनेंट आवासीय, IoT और BTR परिवेशों के लिए वेंडर-न्यूट्रल कार्यान्वयन रणनीतियाँ प्रदान करती है।
प्रति-डिवाइस PSK (iPSK, DPSK, MPSK) का उपयोग करके WiFi SSID की संख्या कैसे कम करें
यह आधिकारिक तकनीकी संदर्भ गाइड बताती है कि कैसे IT टीमें प्रति-डिवाइस PSK (xPSK) का उपयोग करके कई विशिष्ट उद्देश्यों के लिए बनाए गए नेटवर्क को एक सिंगल SSID में मिलाकर SSID बीकन ओवरहेड के कारण होने वाले WiFi परफॉर्मेंस के नुकसान को समाप्त कर सकती हैं। इसमें Cisco iPSK, HPE Aruba MPSK, Ruckus DPSK, Juniper Mist PPSK और Ubiquiti UniFi PPSK के वेंडर परिदृश्य को शामिल किया गया है, जिसमें डायनेमिक VLAN असाइनमेंट, IoT ऑनबोर्डिंग और PCI DSS अनुपालन पर व्यावहारिक कार्यान्वयन मार्गदर्शन दिया गया है। हॉस्पिटैलिटी, रिटेल, स्टेडियम और सार्वजनिक क्षेत्र के संगठनों के वेन्यू ऑपरेटरों को इसमें व्यावहारिक आर्किटेक्चर मार्गदर्शन और वास्तविक दुनिया के व्यावहारिक उदाहरण मिलेंगे।
अपने विशिष्ट सेटअप को लेकर कोई सवाल हैं?
हमारी टीम 80,000 से अधिक वेन्यू में वेन्यू ऑपरेटरों, IT मैनेजरों और नेटवर्क इंजीनियरों के साथ काम करती है। 20 मिनट का कॉल बुक करें और हम आपको दिखाएंगे कि आपके जैसे अन्य लोगों ने इसे कैसे हल किया।