NHS Staff WiFi: Como Implementar Redes Sem Fios Seguras na Saúde
Este guia de referência técnica detalha a arquitetura, os protocolos de segurança e as estratégias de implementação para o NHS Staff WiFi, abrangendo a autenticação 802.1X, segmentação de VLAN, políticas de BYOD e conformidade com o DSP Toolkit. Fornece orientações práticas para líderes de TI sobre a implementação de redes sem fios de nível empresarial que servem utilizadores clínicos, administrativos e convidados numa infraestrutura física partilhada sem comprometer a segurança. Quer esteja a planear uma nova implementação ou a reforçar um parque existente, este guia fornece as estruturas de decisão e as etapas de implementação necessárias para agir este trimestre.
Ouça este guia
Ver transcrição do podcast
📚 Parte da nossa série principal: Enterprise WiFi Security Guide →

कार्यकारी सारांश
NHS संपत्तियों में सुरक्षित, विश्वसनीय WiFi तैनात करना अब कोई वैकल्पिक सुविधा नहीं है — यह एक महत्वपूर्ण नैदानिक बुनियादी ढांचा (clinical infrastructure) है। मोबाइल-फर्स्ट रोगी देखभाल, इलेक्ट्रॉनिक स्वास्थ्य रिकॉर्ड (EHR), और जुड़े हुए चिकित्सा उपकरणों की ओर बढ़ता झुकाव एक ऐसे वायरलेस आर्किटेक्चर की मांग करता है जो कड़े सुरक्षा नियंत्रणों के साथ निर्बाध रोमिंग को संतुलित करे।
IT प्रबंधकों, नेटवर्क आर्किटेक्ट्स और CTOs के लिए, मुख्य चुनौती सुरक्षा से समझौता किए बिना साझा भौतिक बुनियादी ढांचे पर विभिन्न उपयोगकर्ता समूहों — नैदानिक कर्मचारियों, प्रशासनिक कर्मियों, रोगियों और मेहमानों — को समायोजित करना है, जो NHS डेटा सुरक्षा और संरक्षण (DSP) टूलकिट आवश्यकताओं को पूरा करता हो। यह मार्गदर्शिका NHS स्टाफ WiFi के लिए तकनीकी आवश्यकताओं का विवरण देती है, जिसमें IEEE 802.1X जैसे मजबूत प्रमाणीकरण ढांचे, VLANs के माध्यम से तार्किक नेटवर्क विभाजन (logical network segmentation), और Bring Your Own Device (BYOD) एंडपॉइंट्स के सुरक्षित ऑनबोर्डिंग पर ध्यान केंद्रित किया गया है।
विरासत (legacy) प्री-शेयर्ड कीज़ (PSK) से दूर जाकर और पहचान-संचालित एक्सेस नीतियों को अपनाकर, स्वास्थ्य सेवा संगठन उल्लंघन के जोखिम को कम कर सकते हैं, परिचालन संबंधी बाधाओं को कम कर सकते हैं, और डिजिटल परिवर्तन कार्यक्रमों के लिए वायरलेस आधार प्रदान कर सकते हैं। इसका व्यावसायिक पक्ष भी उतना ही मजबूत है: हेल्पडेस्क ओवरहेड में कमी, प्रमाणित DSP टूलकिट अनुपालन, और एक ऐसा नेटवर्क जो बिना किसी पूर्ण बुनियादी ढांचे के पुनर्निर्माण के भविष्य के नैदानिक नवाचारों का समर्थन करने में सक्षम हो।
तकनीकी गहन विश्लेषण
प्रमाणीकरण और एक्सेस नियंत्रण
एक सुरक्षित स्वास्थ्य सेवा वायरलेस नेटवर्क की नींव पहचान-आधारित एक्सेस नियंत्रण है। प्री-शेयर्ड कीज़ का उपयोग करने वाले विरासत WPA2-Personal नेटवर्क नैदानिक वातावरण के लिए मौलिक रूप से अनुपयुक्त हैं। वे कोई व्यक्तिगत जवाबदेही प्रदान नहीं करते हैं, कर्मचारियों के जाने पर ऑनबोर्डिंग हटाने की प्रक्रिया को जटिल बनाते हैं, और क्रेडेंशियल के साथ समझौता होने या इच्छित समूह से बाहर साझा किए जाने पर विफलता का एक एकल बिंदु (single point of failure) पेश करते हैं।
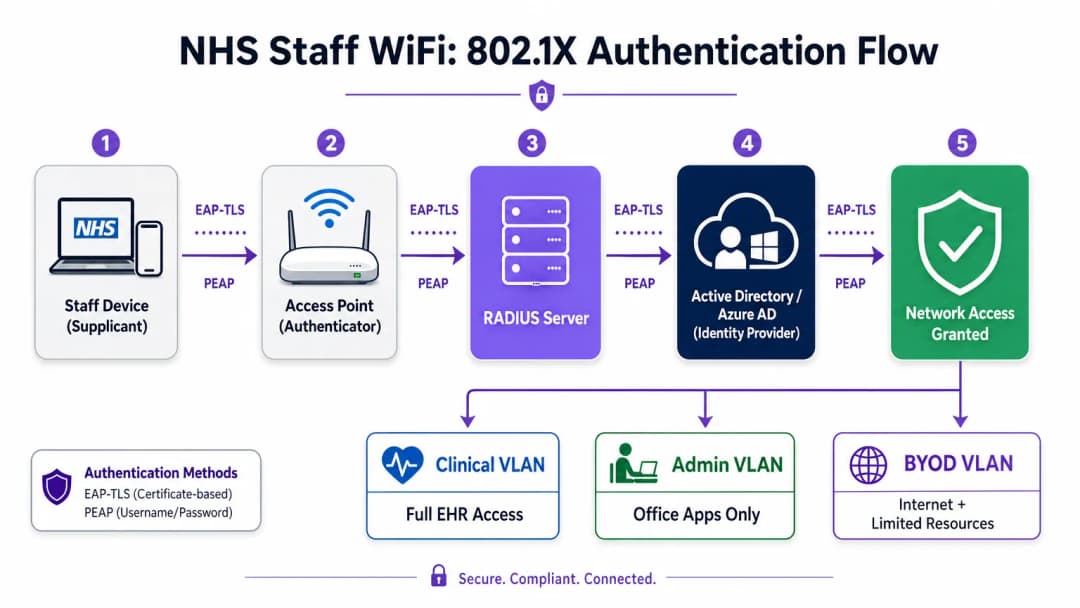
आधुनिक NHS तैनाती में WPA3-Enterprise (या न्यूनतम संक्रमण स्थिति के रूप में WPA2-Enterprise) को IEEE 802.1X प्रमाणीकरण का उपयोग करके अनिवार्य किया जाना चाहिए। इस ढांचे के लिए आवश्यक है कि नेटवर्क एक्सेस दिए जाने से पहले प्रत्येक उपयोगकर्ता या डिवाइस अद्वितीय क्रेडेंशियल प्रस्तुत करे, और उस प्रमाणीकरण का परिणाम यह निर्धारित करता है कि डिवाइस को किस तार्किक नेटवर्क सेगमेंट पर रखा जाए।
स्वास्थ्य सेवा तैनाती में दो EAP तरीके हावी हैं:
| EAP तरीका | प्रमाणीकरण तंत्र | इसके लिए सबसे उपयुक्त | सुरक्षा स्तर |
|---|---|---|---|
| EAP-TLS | क्लाइंट-साइड डिजिटल प्रमाणपत्र | कॉर्पोरेट-प्रबंधित नैदानिक उपकरण | उच्चतम — फ़िशिंग के लिए कोई पासवर्ड नहीं |
| PEAP-MSCHAPv2 | एन्क्रिप्टेड टनल में उपयोगकर्ता नाम/पासवर्ड | BYOD, व्यवस्थापक कर्मचारी, विरासत उपकरण | उच्च — TLS द्वारा सुरक्षित क्रेडेंशियल |
EAP-TLS कॉर्पोरेट उपकरणों के लिए स्वर्ण मानक (gold standard) है। प्रमाणपत्रों को मोबाइल डिवाइस मैनेजमेंट (MDM) प्लेटफॉर्म के माध्यम से वितरित किया जाता है, जिससे ज़ीरो-टच प्रमाणीकरण सक्षम होता है — डिवाइस पृष्ठभूमि में चुपचाप प्रमाणित हो जाता है। PEAP-MSCHAPv2 एक एन्क्रिप्टेड TLS सत्र के भीतर एक्टिव डायरेक्ट्री या एज़्योर AD क्रेडेंशियल को सुरक्षित रूप से टनल करता है, जिससे यह BYOD परिदृश्यों के लिए उपयुक्त हो जाता है जहां प्रमाणपत्र प्रबंधन व्यावहारिक नहीं है।
वायरलेस बुनियादी ढांचे को संगठन के केंद्रीय पहचान प्रदाता (IdP) के साथ एकीकृत करना यह सुनिश्चित करता है कि किसी कर्मचारी का AD खाता अक्षम होने पर एक्सेस स्वचालित रूप से रद्द हो जाए, जो सीधे एक्सेस लाइफसाइकल प्रबंधन के लिए DSP टूलकिट आवश्यकताओं को पूरा करता है।
नेटवर्क विभाजन और ट्रस्ट ज़ोन
भौतिक एक्सेस पॉइंट पूरे अस्पताल के फर्श पर प्रसारण करते हैं, लेकिन तार्किक विभाजन यह सुनिश्चित करता है कि न्यूनतम विशेषाधिकार के सिद्धांत के आधार पर ट्रैफ़िक अलग रहे। स्वास्थ्य सेवा सेटिंग में एक फ्लैट नेटवर्क आर्किटेक्चर एक गंभीर सुरक्षा भेद्यता है, जो एक समझौता किए गए अतिथि डिवाइस या कमजोर IoT सेंसर को संभावित रूप से नैदानिक प्रणालियों तक पहुँचने की अनुमति देता है।
सर्वोत्तम अभ्यास विशिष्ट SSIDs के लिए मैप किए गए अलग वर्चुअल लोकल एरिया नेटवर्क (VLANs) बनाने का निर्देश देता है, जिसमें फ़ायरवॉल नियम उनके बीच ट्रैफ़िक सीमाओं को लागू करते हैं:
| ज़ोन | SSID | प्रमाणीकरण | एक्सेस | QoS प्राथमिकता |
|---|---|---|---|---|
| नैदानिक | NHS-Clinical | EAP-TLS (प्रमाणपत्र) | EHR, PACS, नैदानिक संदेश सेवा | उच्चतम |
| प्रशासनिक | NHS-Staff | PEAP (AD क्रेडेंशियल) | ऑफिस ऐप्स, इंटरनेट | मध्यम |
| मेडिकल IoT | Hidden/MAB | MAC Authentication Bypass | केवल डिवाइस कंट्रोलर | उच्च |
| अतिथि / रोगी | NHS-Guest | Captive Portal | केवल इंटरनेट | निम्न |
| BYOD | NHS-BYOD | PEAP (AD क्रेडेंशियल) | इंटरनेट, सीमित VDI | निम्न |
मेडिकल IoT VLAN विशेष ध्यान देने योग्य है। कई जुड़े हुए चिकित्सा उपकरण — इन्फ्यूजन पंप, रोगी मॉनिटर, वायरलेस कॉल सिस्टम — 802.1X का समर्थन नहीं कर सकते हैं। MAC Authentication Bypass (MAB) इसका विकल्प है, लेकिन इसे सख्त फ़ायरवॉल एक्सेस कंट्रोल लिस्ट (ACLs) के साथ जोड़ा जाना चाहिए जो इन उपकरणों को केवल उनके निर्दिष्ट प्रबंधन सर्वर के साथ संचार करने तक सीमित करते हैं।
BYOD की चुनौती
Bring Your Own Device नीतियां प्रशासनिक कर्मचारियों और आने वाले चिकित्सकों के लिए तेजी से आम हो रही हैं। हालांकि, अप्रबंधित व्यक्तिगत उपकरण एक महत्वपूर्ण जोखिम का प्रतिनिधित्व करते हैं यदि उन्हें विश्वसनीय नेटवर्क सेगमेंट पर जाने की अनुमति दी जाती है।
एक सुरक्षित BYOD तैनाती में इन उपकरणों को एक समर्पित BYOD VLAN पर ऑनबोर्ड करना शामिल है। यह ज़ोन इंटरनेट एक्सेस प्रदान करता है और शायद एक सुरक्षित गेटवे या वर्चुअल डेस्कटॉप इंफ्रास्ट्रक्चर (VDI) के माध्यम से विशिष्ट, गैर-संवेदनशील आंतरिक संसाधनों तक सीमित पहुंच प्रदान करता है। इसमें नैदानिक प्रणालियों या रोगी डेटा स्टोर के लिए सीधे रूटिंग की अनुमति बिल्कुल नहीं होनी चाहिए।

कार्यान्वयन मार्गदर्शिका
एक सुरक्षित NHS स्टाफ WiFi आर्किटेक्चर को तैनात करने के लिए चल रहे नैदानिक संचालन में व्यवधान को कम करने के लिए चरणबद्ध दृष्टिकोण की आवश्यकता होती है।
चरण 1: मूल्यांकन और डिज़ाइन
एक व्यापक वायरलेस साइट सर्वेक्षण के साथ शुरुआत करें। लीड-लाइनेड दीवारों, भारी मशीनरी और घनी आबादी के कारण स्वास्थ्य सेवा वातावरण रेडियो फ्रीक्वेंसी (RF) प्रसार के लिए कुख्यात रूप से कठिन हैं। डिज़ाइन में केवल कवरेज ही नहीं, बल्कि क्षमता का भी ध्यान रखा जाना चाहिए, जिससे आपातकालीन विभागों और बाह्य रोगी क्लीनिकों जैसे उच्च-यातायात वाले क्षेत्रों में पर्याप्त एक्सेस पॉइंट घनत्व सुनिश्चित हो सके।
आवश्यक SSIDs को परिभाषित करें और उन्हें संबंधित VLANs और सुरक्षा नीतियों से मैप करें। प्रसारण SSIDs की संख्या को न्यूनतम रखें — आदर्श रूप से चार से अधिक नहीं — ताकि प्रबंधन ओवरहेड को कम किया जा सके और बीकन फ्रेम कंजेशन को कम किया जा सके, जो समग्र नेटवर्क प्रदर्शन को कम करता है।
चरण 2: बुनियादी ढांचा कॉन्फ़िगरेशन
परिभाषित VLANs का समर्थन करने के लिए कोर स्विचिंग और रूटिंग बुनियादी ढांचे को कॉन्फ़िगर करें। न्यूनतम विशेषाधिकार लागू करने के लिए सेगमेंट के बीच की सीमाओं पर फ़ायरवॉल नियम लागू करें। RADIUS सर्वर (जैसे, Cisco ISE, Aruba ClearPass, या क्लाउड-आधारित RADIUS-as-a-Service) सेट करें और इसे केंद्रीय पहचान प्रदाता के साथ एकीकृत करें। जिन वातावरणों में Purple का प्लेटफ़ॉर्म तैनात है, वहां इस चरण में WiFi Analytics को एकीकृत करना नेटवर्क उपयोग, रोमिंग पैटर्न और क्षमता हॉटस्पॉट में दृश्यता प्रदान करता है।
चरण 3: नीति प्रवर्तन और ऑनबोर्डिंग
प्रमाणीकरण नीतियां तैनात करें। कॉर्पोरेट उपकरणों के लिए, आवश्यक वायरलेस प्रोफाइल और क्लाइंट प्रमाणपत्र (EAP-TLS के लिए) भेजने के लिए MDM समाधान का उपयोग करें। यह सुनिश्चित करता है कि प्रबंधित उपकरण उपयोगकर्ता के हस्तक्षेप के बिना स्वचालित रूप से और सुरक्षित रूप से कनेक्ट हों।
BYOD के लिए, एक स्पष्ट ऑनबोर्डिंग वर्कफ़्लो स्थापित करें — आमतौर पर एक ऑनबोर्डिंग पोर्टल जो उपयोगकर्ता को उनके कॉर्पोरेट क्रेडेंशियल के साथ प्रमाणित करने, स्वीकार्य उपयोग नीति को स्वीकार करने और डिवाइस को सुरक्षित BYOD VLAN पर ले जाने के माध्यम से मार्गदर्शन करता है। Purple के Guest WiFi प्लेटफ़ॉर्म को रोगी और अतिथि SSID के लिए Captive Portal परत के रूप में तैनात किया जा सकता है, जो बड़े पैमाने पर GDPR-अनुरूप डेटा कैप्चर और शर्तों की स्वीकृति को संभालता है।
चरण 4: परीक्षण और सत्यापन
गो-लाइव से पहले, प्रत्येक प्रमाणीकरण पथ, VLAN असाइनमेंट और फ़ायरवॉल नियम का एंड-टू-एंड परीक्षण करें। विशेष रूप से पुनः प्रमाणीकरण घटनाओं की निगरानी करते हुए एक परीक्षण डिवाइस के साथ नैदानिक फर्श पर चलकर रोमिंग व्यवहार को मान्य करें। पुष्टि करें कि फास्ट रोमिंग प्रोटोकॉल (802.11r और 802.11k) सही ढंग से काम कर रहे हैं और एप्लिकेशन सत्र AP संक्रमणों के बाद भी बने रहते हैं।
सर्वोत्तम अभ्यास
प्री-शेयर्ड कीज़ को समाप्त करें। व्यक्तिगत जवाबदेही और केंद्रीकृत एक्सेस नियंत्रण सुनिश्चित करने के लिए सभी कर्मचारियों और नैदानिक नेटवर्क को 802.1X प्रमाणीकरण पर स्थानांतरित करें। यह DSP टूलकिट अनुपालन के लिए एक गैर-परक्राम्य आवश्यकता है।
सख्त विभाजन लागू करें। अतिथि, BYOD, या IoT ट्रैफ़िक को कभी भी नैदानिक डेटा के समान तार्किक सेगमेंट पर अनुमति न दें। डिफ़ॉल्ट नीति के रूप में स्पष्ट अस्वीकार (deny) नियमों के साथ, इंटर-VLAN रूटिंग को नियंत्रित करने के लिए स्टेटफुल फ़ायरवॉल का उपयोग करें।
नैदानिक ट्रैफ़िक को प्राथमिकता दें। विशेष रूप से उच्च भीड़ की अवधि के दौरान, अतिथि या प्रशासनिक ट्रैफ़िक की तुलना में नैदानिक अनुप्रयोगों — वॉयस ओवर WLAN, EHR एक्सेस — को प्राथमिकता देने के लिए वायरलेस कंट्रोलर और स्विच पर QoS नीतियां लागू करें।
फास्ट रोमिंग सक्षम करें। 802.11r (फास्ट BSS ट्रांज़िशन) और 802.11k (रेडियो रिसोर्स मेजरमेंट) को तैनात करें ताकि यह सुनिश्चित हो सके कि नैदानिक कर्मचारी एप्लिकेशन टाइमआउट या टूटे हुए कनेक्शन का अनुभव किए बिना सुविधा के माध्यम से आगे बढ़ सकें।
निरंतर निगरानी। नेटवर्क स्वास्थ्य की निगरानी करने, अनधिकृत एक्सेस पॉइंट की पहचान करने और उपयोगकर्ता रोमिंग व्यवहार को ट्रैक करने के लिए एनालिटिक्स प्लेटफॉर्म का उपयोग करें। फुटफॉल और उपयोग के पैटर्न को समझना — Retail और Hospitality वातावरण में सिद्ध एक तकनीक — क्षमता योजना और समस्या निवारण के लिए अस्पताल की सेटिंग में भी उतनी ही मूल्यवान है।
नियमित ऑडिटिंग। जहां लागू हो, DSP टूलकिट, साइबर एसेंशियल प्लस और ISO 27001 के साथ निरंतर अनुपालन सुनिश्चित करने के लिए वार्षिक वायरलेस जोखिम मूल्यांकन आयोजित करें।
समस्या निवारण और जोखिम शमन
प्रमाणीकरण टाइमआउट
उच्च क्लाइंट घनत्व वाले वातावरण में, RADIUS सर्वर अभिभूत हो सकते हैं, जिससे प्रमाणीकरण टाइमआउट और टूटे हुए कनेक्शन हो सकते हैं। सुनिश्चित करें कि RADIUS बुनियादी ढांचा पर्याप्त रूप से स्केल किया गया है और अत्यधिक उपलब्ध है। कई प्रमाणीकरण सर्वरों में लोड बैलेंसिंग लागू करें और एक प्रमुख परिचालन मीट्रिक के रूप में RADIUS प्रतिक्रिया समय की निगरानी करें।
रोमिंग के मुद्दे
वार्डों के बीच तेजी से चलने वाले नैदानिक कर्मचारियों को टूटे हुए कनेक्शन का अनुभव हो सकता है यदि वायरलेस बुनियादी ढांचा फास्ट रोमिंग प्रोटोकॉल का समर्थन नहीं करता है। वायरलेस कंट्रोलर पर 802.11r और 802.11k सक्षम करें और सुनिश्चित करें कि क्लाइंट डिवाइस इन मानकों का समर्थन करते हैं। कवरेज अंतराल या 'स्टिकी क्लाइंट' मुद्दों की पहचान करने और उन्हें हल करने के लिए पोस्ट-डिप्लॉयमेंट रोमिंग सर्वेक्षण आयोजित करें, जहां एक डिवाइस करीब जाने के बजाय दूर के, कमजोर AP से चिपका रहता है।
विरासत डिवाइस असंगतता
पुराने चिकित्सा उपकरण WPA3 या 802.1X जैसे आधुनिक सुरक्षा प्रोटोकॉल का समर्थन नहीं कर सकते हैं। MAB का उपयोग करके इन उपकरणों को एक समर्पित IoT VLAN पर अलग करें। उनके संचार को केवल आवश्यक प्रबंधन सर्वर तक सीमित करने के लिए सख्त फ़ायरवॉल नियम लागू करें। उन महत्वपूर्ण उपकरणों के लिए हार्डवेयर अपग्रेड या वायरलेस ब्रिज पर विचार करें जिन्हें मूल रूप से सुरक्षित नहीं किया जा सकता है।
प्रमाणपत्र की समाप्ति
EAP-TLS तैनाती परिभाषित समाप्ति अवधि वाले प्रमाणपत्रों पर निर्भर करती है। यदि प्रमाणपत्र नवीनीकरण के बिना समाप्त हो जाते हैं, तो डिवाइस प्रमाणित करने में विफल हो जाएंगे, जिससे व्यापक नैदानिक व्यवधान होगा। MDM प्लेटफॉर्म के माध्यम से SCEP (सिंपल सर्टिफिकेट एनरोलमेंट प्रोटोकॉल) के माध्यम से स्वचालित प्रमाणपत्र नवीनीकरण लागू करें, और सक्रिय रूप से प्रमाणपत्र समाप्ति तिथियों की निगरानी करें।
ROI और व्यावसायिक प्रभाव
एक सुरक्षित, एंटरप्राइज़-ग्रेड वायरलेस आर्किटेक्चर में निवेश नैदानिक, परिचालन और IT डोमेन में मापने योग्य रिटर्न प्रदान करता है।
नैदानिक दक्षता। विश्वसनीय कनेक्टिविटी यह सुनिश्चित करती है कि चिकित्सकों के पास देखभाल के बिंदु पर रोगी के रिकॉर्ड तक तत्काल पहुंच हो, जिससे जानकारी खोजने या टूटे हुए कनेक्शन से निपटने में लगने वाला समय कम हो जाता है। यह सीधे रोगी थ्रूपुट और देखभाल वितरण की गुणवत्ता को प्रभावित करता है।
कम IT ओवरहेड। साझा पासवर्ड और मैन्युअल ऑनबोर्डिंग से हटकर स्वचालित, प्रमाणपत्र-आधारित प्रमाणीकरण की ओर बढ़ने से पासवर्ड रीसेट और कनेक्टिविटी समस्याओं से संबंधित हेल्पडेस्क टिकटों में काफी कमी आती है। एक NHS ट्रस्ट ने 802.1X पर माइग्रेशन के बाद वायरलेस से संबंधित हेल्पडेस्क कॉल में 40% की कमी दर्ज की।
जोखिम शमन। सख्त विभाजन और मजबूत प्रमाणीकरण DSP टूलकिट आवश्यकताओं को पूरा करने, डेटा उल्लंघनों या अनुपालन विफलताओं से जुड़े वित्तीय और प्रतिष्ठित जोखिमों को कम करने के लिए मौलिक हैं। डेटा उल्लंघन की लागत उचित रूप से तैयार की गई वायरलेस संपत्ति में निवेश से कहीं अधिक है।
भविष्य के लिए तैयार करना (Future-Proofing)। एक अच्छी तरह से डिज़ाइन किया गया वायरलेस नेटवर्क भविष्य की डिजिटल स्वास्थ्य पहलों — स्थान-आधारित सेवाएं, रीयल-टाइम एसेट ट्रैकिंग, उन्नत टेलीहेल्थ एप्लिकेशन — के लिए आधार प्रदान करता है, जो Healthcare और Transport जैसे संबंधित क्षेत्रों में व्यापक रणनीतिक लक्ष्यों के साथ संरेखित होता है जहां मोबाइल कनेक्टिविटी परिचालन दक्षता को रेखांकित करती है।
उन संगठनों के लिए जो यह समझना चाहते हैं कि Purple का प्लेटफ़ॉर्म इस आर्किटेक्चर के अतिथि और रोगी WiFi परत से कैसे मेल खाता है, Healthcare उद्योग पृष्ठ NHS-संगत Captive Portal, एनालिटिक्स और GDPR-अनुरूप डेटा हैंडलिंग क्षमताओं का एक विस्तृत अवलोकन प्रदान करता है। वही एनालिटिक्स सिद्धांत जो Retail में ग्राहक जुड़ाव को बढ़ावा देते हैं, सीधे अस्पताल संपदा टीमों के लिए परिचालन खुफिया में अनुवादित होते हैं।
Definições Principais
IEEE 802.1X
Um padrão IEEE para Controlo de Acesso à Rede baseado em portas (PNAC). Fornece um mecanismo de autenticação para dispositivos que pretendem ligar-se a uma LAN ou WLAN, exigindo que cada dispositivo apresente credenciais antes de lhe ser concedido acesso.
Este é o padrão obrigatório para substituir palavras-passe partilhadas inseguras por inícios de sessão individuais, baseados na identidade, para funcionários e dispositivos clínicos. É a pedra angular de uma arquitetura sem fios em conformidade com o DSP Toolkit.
VLAN (Virtual Local Area Network)
Uma sub-rede lógica que agrupa uma coleção de dispositivos de diferentes segmentos de rede física. As VLANs permitem que os administradores de rede particionem uma única rede comutada para corresponder aos requisitos funcionais e de segurança de diferentes grupos de utilizadores.
As VLANs são essenciais para segmentar o tráfego clínico do tráfego de convidados e administrativo, limitando o raio de impacto de uma potencial violação de segurança e aplicando o princípio do privilégio mínimo.
RADIUS (Remote Authentication Dial-In User Service)
Um protocolo de rede que fornece gestão centralizada de Autenticação, Autorização e Contabilização (AAA) para utilizadores que se ligam e utilizam um serviço de rede.
O servidor RADIUS atua como o motor de decisão entre os pontos de acesso sem fios e a base de dados de identidade central (Active Directory), decidindo quem obtém acesso e a que VLAN é atribuído.
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
Um método EAP que depende de certificados de cliente e servidor para estabelecer uma ligação segura e mutuamente autenticada. Nenhuma das partes confia na outra sem um certificado válido.
O método mais seguro para autenticar dispositivos pertencentes ao hospital. Os certificados distribuídos via MDM garantem que apenas endpoints geridos e fidedignos podem aceder à rede clínica, sem palavras-passe para phish ou partilhar.
MAB (MAC Authentication Bypass)
Um método de autenticação de dispositivos com base no seu endereço MAC de hardware, utilizado como alternativa para dispositivos que não suportam 802.1X.
Necessário para dispositivos IoT médicos legados que precisam de acesso à rede mas não conseguem processar protocolos de autenticação complexos. Deve ser sempre emparelhado com ACLs de firewall estritas para conter o dispositivo nos seus caminhos de comunicação permitidos.
DSP Toolkit (Data Security and Protection Toolkit)
Uma ferramenta de autoavaliação online mandatada pelo NHS England que todas as organizações devem preencher se tiverem acesso a dados e sistemas de doentes do NHS. Alinha-se com os dez padrões de segurança de dados do National Data Guardian.
A conformidade com o DSP Toolkit é obrigatória para as organizações do NHS e respetivos fornecedores. Uma segurança sem fios robusta — incluindo 802.1X, segmentação e gestão do ciclo de vida dos acessos — é um componente crítico para demonstrar a conformidade.
SSID (Service Set Identifier)
O nome principal associado a uma rede local sem fios 802.11, transmitido por pontos de acesso para permitir que os dispositivos clientes identifiquem e se liguem à rede.
Os hospitais devem minimizar o número de SSIDs transmitidos (ex: NHS-Clinical, NHS-Guest) para reduzir a sobrecarga de gestão e de RF. Cada SSID deve mapear para uma política de segurança e VLAN específicas.
QoS (Quality of Service)
Tecnologias que gerem o tráfego de dados para reduzir a perda de pacotes, a latência e o jitter numa rede, priorizando certos tipos de tráfego sobre outros.
Crucial na área da saúde para garantir que as aplicações clínicas críticas para a vida e as comunicações de voz têm sempre prioridade sobre o tráfego menos importante, como a transmissão de vídeo de convidados ou atualizações de software.
802.11r (Fast BSS Transition)
Uma emenda IEEE que permite o roaming rápido entre pontos de acesso através da pré-autenticação do cliente no AP de destino antes que a transição física ocorra, reduzindo drasticamente a latência de roaming.
Essencial para ambientes clínicos onde os funcionários estão em constante movimento. Sem o 802.11r, os dispositivos têm de realizar uma reautenticação RADIUS completa em cada transição de AP, o que pode causar a expiração das sessões das aplicações.
Exemplos Práticos
Um NHS Trust está a implementar novas estações de trabalho móveis (Workstations on Wheels) em várias enfermarias. A equipa de TI precisa de garantir que estes dispositivos mantêm a conectividade à medida que os enfermeiros se deslocam entre pontos de acesso, garantindo também que apenas dispositivos autorizados podem aceder à VLAN clínica que contém o sistema de Registo de Saúde Eletrónico.
O Trust deve implementar uma estrutura de autenticação 802.1X utilizando EAP-TLS. A equipa de TI utilizará a sua solução MDM para enviar um certificado de cliente exclusivo e o perfil sem fios correspondente para cada estação de trabalho. Os controladores sem fios serão configurados para autenticar estes dispositivos num servidor RADIUS, que verifica o certificado em relação à PKI interna. Após a autenticação bem-sucedida, o servidor RADIUS atribui dinamicamente a estação de trabalho à VLAN Clínica dedicada através de um atributo RADIUS (por exemplo, Tunnel-Private-Group-ID). Para responder ao requisito de roaming, o 802.11r (Fast BSS Transition) e o 802.11k (Radio Resource Measurement) devem ser ativados na infraestrutura sem fios para permitir que as estações de trabalho transitem perfeitamente entre pontos de acesso sem realizar um ciclo completo de nova autenticação no servidor RADIUS de cada vez.
Um hospital precisa de fornecer acesso à internet para médicos tarefeiros visitantes que utilizam os seus portáteis pessoais (BYOD). Estes médicos precisam de aceder a ferramentas de referência médica baseadas na nuvem, mas devem ser estritamente proibidos de aceder às bases de dados internas de doentes do hospital.
O hospital deve implementar um SSID BYOD dedicado mapeado para uma VLAN BYOD isolada. A autenticação deve ser gerida através de 802.1X utilizando PEAP-MSCHAPv2, permitindo que os tarefeiros iniciem sessão utilizando credenciais temporárias do Active Directory fornecidas pelos Recursos Humanos à chegada. O firewall principal deve ser configurado com uma ACL que negue explicitamente qualquer encaminhamento da VLAN BYOD para as VLANs Clínicas ou Administrativas, permitindo apenas tráfego de saída para a internet. Adicionalmente, um Captive Portal pode ser utilizado na ligação inicial para impor uma Política de Utilização Aceitável antes de conceder acesso total à internet. Quando a conta temporária de AD do tarefeiro for desativada no final do seu contrato, o seu acesso sem fios é automaticamente revogado.
Perguntas de Prática
Q1. Uma nova ala está a ser adicionada ao hospital e a equipa de instalações pretende implementar sensores de temperatura sem fios nos frigoríficos de armazenamento de medicamentos. Estes sensores apenas suportam WPA2-Personal (Pre-Shared Key) e não podem utilizar 802.1X. Como deve o arquiteto de rede integrá-los de forma segura?
Dica: Considere o princípio do privilégio mínimo e como isolar dispositivos não conformes dos sistemas clínicos.
Ver resposta modelo
O arquiteto deve criar um SSID dedicado e oculto, mapeado para uma VLAN específica "Facilities IoT". Os sensores ligar-se-ão utilizando a PSK. Crucialmente, devem ser aplicadas ACLs de firewall rigorosas a esta VLAN, permitindo que os sensores comuniquem apenas com o seu servidor de gestão central específico e negando todo o restante tráfego — particularmente o encaminhamento para a VLAN Clínica ou para a internet. O MAC Authentication Bypass (MAB) também deve ser configurado para garantir que apenas os endereços MAC específicos dos sensores adquiridos sejam permitidos nessa VLAN, impedindo que dispositivos não autorizados se juntem utilizando a mesma PSK.
Q2. Durante um turno da manhã movimentado, os enfermeiros relatam que os seus tablets perdem frequentemente a ligação ao sistema EHR enquanto percorrem a enfermaria, obrigando-os a iniciar sessão novamente. O levantamento da cobertura sem fios mostra uma forte intensidade de sinal em toda a enfermaria. Qual é a causa provável e a solução?
Dica: Um sinal forte não garante transições fluidas entre pontos de acesso. Considere o processamento de autenticação em cada transição de AP.
Ver resposta modelo
A causa provável é a falta de protocolos de roaming rápido. À medida que o tablet se move para fora do alcance de um AP e se liga ao seguinte, é forçado a realizar uma reautenticação 802.1X completa contra o servidor RADIUS, o que introduz latência suficiente para fazer com que a sessão da aplicação EHR expire. A solução é ativar o 802.11r (Fast BSS Transition) nos controladores sem fios, o que permite ao cliente fazer roaming de forma segura entre APs sem a latência de um ciclo de reautenticação completo. O 802.11k também deve ser ativado para ajudar o dispositivo a identificar o AP de destino ideal antes que a transição ocorra.
Q3. Um NHS Trust está a preparar-se para a sua avaliação anual do DSP Toolkit. O auditor nota que a equipa administrativa utiliza uma palavra-passe partilhada para aceder à rede Staff WiFi. Qual é o principal risco identificado aqui e qual é a remediação recomendada?
Dica: Foque-se na responsabilidade individual e no ciclo de vida do acesso quando os colaboradores deixam a organização.
Ver resposta modelo
O principal risco é a falta de responsabilidade individual e uma gestão deficiente do ciclo de vida dos acessos. Se um membro da equipa administrativa deixar o Trust, a palavra-passe partilhada permanece válida, permitindo potencialmente o acesso não autorizado. Além disso, é impossível auditar qual o utilizador específico que realizou uma ação na rede. A remediação consiste em descontinuar a rede de palavra-passe partilhada (PSK) e migrar a equipa administrativa para uma rede autenticada por 802.1X utilizando PEAP-MSCHAPv2 com as suas credenciais do Active Directory. Isto garante a responsabilidade individual e a revogação automática do acesso quando a sua conta AD é desativada após a saída, respondendo diretamente aos requisitos do DSP Toolkit para controlo de acessos e registo de auditoria.
Continue a ler esta série
Compreender o Cisco SUDI: Identidade Ancorada em Hardware no Controlo de Acesso Seguro à Rede
Este guia explica como o Cisco SUDI fornece uma identidade criptograficamente segura e ancorada em hardware para a infraestrutura de rede empresarial. Saiba como substituir endereços MAC clonáveis por certificados 802.1AR imutáveis para proteger o controlo de acesso à rede do seu espaço.
How to Configure SCEP for Automated Enterprise WiFi Certificate Enrollment
Este guia explica como configurar o SCEP (Simple Certificate Enrollment Protocol) para a atribuição automatizada de certificados WiFi empresariais, cobrindo toda a arquitetura desde PKI e NDES até à implementação de perfis MDM e validação RADIUS. Destina-se a gestores de TI, arquitetos de rede e CTOs em hotéis, cadeias de retalho, estádios, centros de conferências e organizações do setor público que necessitam de ir além das chaves pré-partilhadas e implementar uma autenticação 802.1X EAP-TLS escalável e baseada em identidade. A plataforma de sobreposição na nuvem da Purple, independente de hardware, integra-se diretamente com esta arquitetura, fornecendo a camada de WiFi para convidados e BYOD que coexiste com a sua rede de colaboradores autenticada por certificado.
Como Implementar SCEP para a Inscrição Automatizada de Certificados WiFi
Este guia explica como implementar o SCEP (Simple Certificate Enrollment Protocol) para a inscrição automatizada de certificados WiFi em espaços empresariais. Abrange todo o plano de arquitetura - desde o design de PKI e integração de MDM até à sequência de implementação obrigatória de três passos - e mostra aos gestores de TI e arquitetos de rede como eliminar credenciais partilhadas, automatizar a gestão do ciclo de vida dos certificados e cumprir os requisitos de PCI DSS e GDPR à escala.