Healthcare WiFi: HIPAA, DSPT and WiFi Compliance Explained
Este guia fornece uma referência técnica definitiva para gestores de TI, arquitetos de rede e responsáveis de conformidade que implementam redes sem fios em ambientes de saúde. Mapeia os requisitos específicos do HIPAA (EUA) e do NHS Data Security and Protection Toolkit (DSPT, Reino Unido) para decisões concretas de arquitetura de rede — abrangendo segmentação, acesso baseado em identidade, padrões de encriptação e gestão de dispositivos IoMT. A plataforma de WiFi de convidados e analítica da Purple é posicionada ao longo do documento como uma solução de classe empresarial em conformidade para gerir a conectividade de doentes e visitantes dentro de um património sem fios governado.
Ouça este guia
Ver transcrição do podcast
📚 Parte da nossa série principal: Enterprise WiFi Security Guide →
कार्यकारी सारांश
हेल्थकेअर WiFi कंप्लायन्स हे केवळ कॉन्फिगरेशन सेटिंग नाही — ती एक आर्किटेक्चरल शिस्त आहे. तुमची संस्था युनायटेड स्टेट्समधील HIPAA अंतर्गत किंवा युनायटेड किंगडममधील NHS डेटा सिक्युरिटी अँड प्रोटेक्शन टूलकिट (DSPT) अंतर्गत कार्यरत असली तरीही, नियामक अपेक्षा समान आहे: तुमच्या वायरलेस इस्टेटवरील प्रत्येक डिव्हाइस, प्रत्येक वापरकर्ता आणि प्रत्येक डेटा फ्लोचा हिशेब, नियंत्रण आणि ऑडिट होणे आवश्यक आहे.
यूएस मध्ये हेल्थकेअर डेटा ब्रीचची सरासरी किंमत आता प्रति घटना $10.9 दशलक्ष पेक्षा जास्त आहे, ज्यामुळे सलग तेराव्या वर्षी ब्रीचसाठी हे सर्वात महागडे क्षेत्र बनले आहे. यूके मध्ये, NHS ट्रस्ट जे त्यांचे वार्षिक DSPT सबमिशन पूर्ण करण्यात अपयशी ठरतात त्यांना राष्ट्रीय सिस्टीमचा ॲक्सेस गमावावा लागतो आणि अनिवार्य सुधारणा कार्यक्रमांना सामोरे जावे लागते. वायरलेस नेटवर्क हा सहसा दोन्ही वातावरणातील सर्वात कमकुवत दुवा असतो — तंत्रज्ञान अपुरे असल्यामुळे नाही, तर कंप्लायन्स फ्रेमवर्क लक्षात न ठेवता डिप्लॉयमेंटचे निर्णय घेतल्यामुळे.
या मार्गदर्शकामध्ये तांत्रिक आर्किटेक्चर, रेग्युलेटरी मॅपिंग आणि दोन्ही फ्रेमवर्क पूर्ण करणारे healthcare -ग्रेड वायरलेस नेटवर्क डिप्लॉय करण्यासाठी आवश्यक असलेल्या अंमलबजावणीच्या टप्प्यांचा समावेश आहे. हे रुग्ण आणि अभ्यागत guest WiFi च्या विशिष्ट आव्हानाला देखील संबोधित करते — एक सेवा जी एकाच वेळी ॲक्सेसिबल, कंप्लायंट आणि क्लिनिकल सिस्टीमपासून पूर्णपणे वेगळी असणे आवश्यक आहे.

तांत्रिक सखोल माहिती (Technical Deep-Dive)
नियामक परिदृश्य (The Regulatory Landscape)
HIPAA चा सिक्युरिटी नियम (45 CFR भाग 164) इलेक्ट्रॉनिक संरक्षित आरोग्य माहिती (ePHI) साठी सुरक्षिततेच्या तीन श्रेणी स्थापित करतो: प्रशासकीय, भौतिक आणि तांत्रिक. वायरलेस नेटवर्कसाठी, §164.312 अंतर्गत तांत्रिक सुरक्षा उपाय सर्वात थेट लागू होतात. हे ॲक्सेस कंट्रोल्स (§164.312(a)(1)), ऑडिट कंट्रोल्स (§164.312(b)), इंटिग्रिटी कंट्रोल्स (§164.312(c)(1)), आणि ट्रान्समिशन सिक्युरिटी (§164.312(e)(1)) अनिवार्य करतात. विशेष म्हणजे, सिक्युरिटी नियम तंत्रज्ञान-तटस्थ आहे — तो विशिष्ट प्रोटोकॉल विहित करत नाही, परंतु संस्थांनी मानकांची पूर्तता करणारी यंत्रणा लागू करणे आवश्यक आहे.
NHS DSPT दहा नॅशनल डेटा गार्डियन (NDG) डेटा सिक्युरिटी स्टँडर्ड्सभोवती संरचित आहे. वायरलेस नेटवर्कसाठी, सर्वात संबंधित स्टँडर्ड 1 (वैयक्तिक गोपनीय डेटा केवळ आवश्यक असलेल्या कर्मचाऱ्यांसाठी ॲक्सेसिबल आहे), स्टँडर्ड 6 (सर्व वैयक्तिक डेटा कायदेशीर आणि योग्यरित्या प्रोसेस केला जातो), आणि स्टँडर्ड 9 (असमर्थित सिस्टीम ओळखल्या जातात आणि व्यवस्थापित केल्या जातात) आहेत. DSPT मध्ये सायबर एसेन्शियल्स प्लस आवश्यकता देखील समाविष्ट आहेत, जे नेटवर्क बाउंड्री फायरवॉल, सुरक्षित कॉन्फिगरेशन, ॲक्सेस कंट्रोल, मालवेअर संरक्षण आणि पॅच मॅनेजमेंटसह विशिष्ट तांत्रिक कंट्रोल्स अनिवार्य करतात — या सर्वांचे थेट वायरलेस नेटवर्कवर परिणाम होतात.
दोन फ्रेमवर्कमधील मुख्य फरक अंमलबजावणी यंत्रणा आहे. HIPAA ची अंमलबजावणी HHS ऑफिस फॉर सिव्हिल राइट्स (OCR) द्वारे प्रति उल्लंघन श्रेणी प्रति वर्ष $100 ते $50,000 पर्यंतच्या आर्थिक दंडाद्वारे केली जाते. DSPT कंप्लायन्सची अंमलबजावणी NHS इंग्लंडद्वारे केली जाते, ज्यामध्ये नॉन-कंप्लायंट संस्थांना NHS राष्ट्रीय सिस्टीमचा ॲक्सेस गमावण्याची आणि अनिवार्य सुधारणा योजनांना सामोरे जाण्याची शक्यता असते. दोन्ही फ्रेमवर्कसाठी वार्षिक पुनरावलोकन आणि पुरावे सबमिशन आवश्यक आहे.
नेटवर्क आर्किटेक्चर: चार ट्रस्ट झोन
हेल्थकेअर WiFi कंप्लायन्सचे मूलभूत तत्त्व म्हणजे वेगळ्या ट्रस्ट झोनमध्ये नेटवर्क सेगमेंटेशन. फ्लॅट नेटवर्क — अगदी एकाधिक SSID असलेले — अंतर्निहित पॉलिसी अंमलबजावणी कमकुवत असल्यास कोणत्याही फ्रेमवर्कच्या ॲक्सेस कंट्रोल आवश्यकता पूर्ण करत नाही.
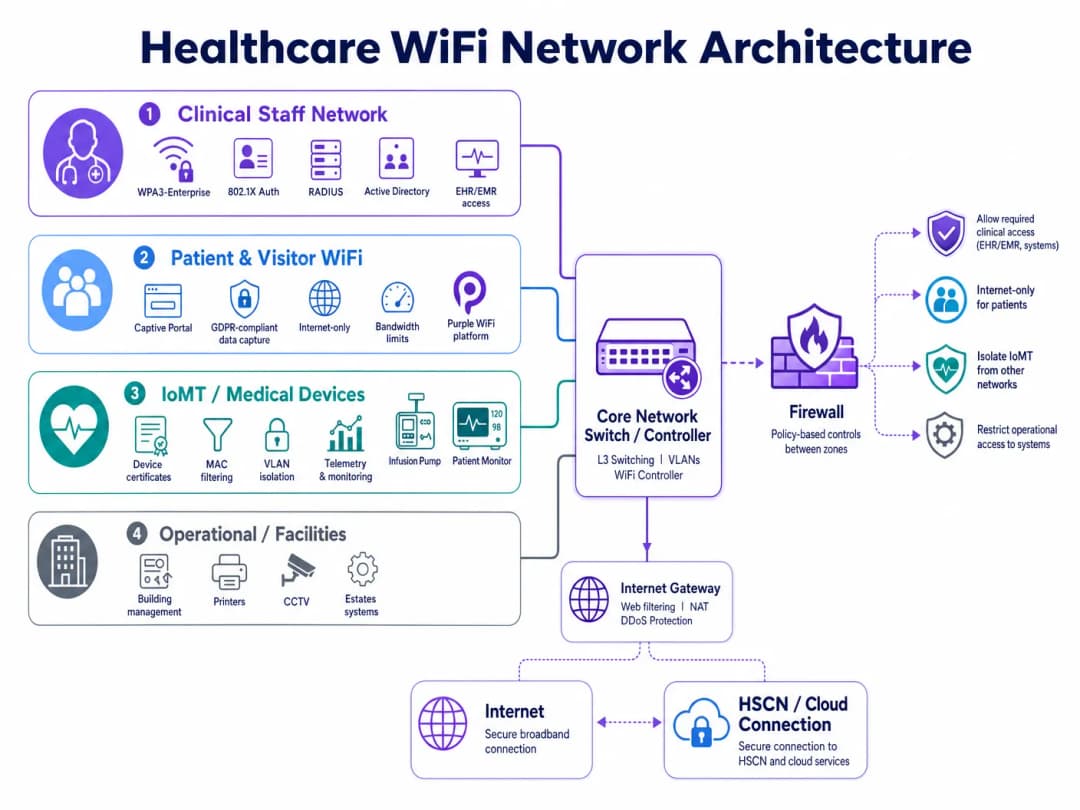
कंप्लायंट हॉस्पिटल वायरलेस इस्टेटसाठी चार भिन्न पॉलिसी डोमेन आवश्यक आहेत:
| झोन | वापरकर्ता/डिव्हाइस प्रकार | ऑथेंटिकेशन पद्धत | ॲक्सेस स्कोप | कंप्लायन्स ड्रायव्हर |
|---|---|---|---|---|
| क्लिनिकल कर्मचारी | क्लिनिशियन, परिचारिका, ॲडमिन | WPA3-Enterprise, 802.1X, RADIUS | EHR/EMR, क्लिनिकल ॲप्स, अंतर्गत सेवा | HIPAA §164.312(a), DSPT स्टँडर्ड 1 |
| रुग्ण आणि अभ्यागत | रुग्ण, कुटुंबे, अभ्यागत | Captive Portal (GDPR-कंप्लायंट) | केवळ इंटरनेट, कोणतेही अंतर्गत राउटिंग नाही | HIPAA §164.312(e), GDPR कलम 5 |
| IoMT / वैद्यकीय उपकरणे | इन्फ्युजन पंप, मॉनिटर्स, टेलिमेट्री | डिव्हाइस सर्टिफिकेट्स, MAC फिल्टरिंग | प्रति डिव्हाइस प्रकार मायक्रो-सेगमेंट केलेले | HIPAA किमान आवश्यक, DSPT स्टँडर्ड 9 |
| ऑपरेशनल / सुविधा | प्रिंटर, CCTV, BMS, इस्टेट्स | समर्पित VLAN, व्यवस्थापित क्रेडेंशियल्स | केवळ ऑपरेशनल सिस्टीम | DSPT स्टँडर्ड 6, HIPAA §164.312(a) |
सेगमेंटेशन नेटवर्क लेयरवर लागू केले जाणे आवश्यक आहे — केवळ SSID लेबलवर नाही. प्रत्येक झोनला स्वतःचे VLAN, समर्पित फायरवॉल पॉलिसी आणि इंटर-झोन ॲक्सेस कंट्रोल लिस्ट (ACLs) आवश्यक आहेत जे डीफॉल्टनुसार डिनाय (deny) करतात. क्लिनिकल कर्मचारी झोनचा गेस्ट झोनकडे कोणताही राउटेबल मार्ग नसावा आणि IoMT झोनमध्ये केवळ विशिष्ट सर्व्हर आणि पोर्ट्सपुरते मर्यादित कम्युनिकेशन मार्ग असणे आवश्यक आहे जे प्रत्येक डिव्हाइस प्रकारासाठी आवश्यक आहेत.
आयडेंटिटी-आधारित ॲक्सेस: शेअर्ड PSKs च्या पलीकडे जाणे
शेअर्ड प्री-शेअर्ड की (PSKs) हेल्थकेअर वायरलेस डिप्लॉयमेंटमध्ये सर्वात सामान्य कंप्लायन्स अपयश राहिल्या आहेत. त्या ऑपरेशनलदृष्ट्या सोयीस्कर आहेत परंतु तीन गंभीर समस्या निर्माण करतात: त्या विशिष्ट वापरकर्ता किंवा डिव्हाइसला नियुक्त केल्या जाऊ शकत नाहीत, कर्मचाऱ्यांच्या टर्नओव्हरशी जुळणाऱ्या वेळापत्रकानुसार त्या क्वचितच रोटेट केल्या जातात आणि जेव्हा एखादा कर्मचारी निघून जातो किंवा डिव्हाइस डिकमिशन केले जाते तेव्हा त्वरित रिव्होकेशनसाठी कोणतीही यंत्रणा प्रदान करत नाहीत.
EAP-TLS (एक्स्टेंसिबल ऑथेंटिकेशन प्रोटोकॉल — ट्रान्सपोर्ट लेयर सिक्युरिटी) सह IEEE 802.1X हे हेल्थकेअरमधील आयडेंटिटी-आधारित वायरलेस ॲक्सेससाठी सध्याचे मानक आहे. या मॉडेल अंतर्गत, प्रत्येक वापरकर्ता किंवा व्यवस्थापित डिव्हाइस संस्थेच्या PKI (पब्लिक की इन्फ्रास्ट्रक्चर) द्वारे जारी केलेले सर्टिफिकेट सादर करते. RADIUS सर्व्हर ॲक्टिव्ह डिरेक्टरी किंवा LDAP डिरेक्टरी विरुद्ध सर्टिफिकेट प्रमाणित करतो, योग्य VLAN आणि पॉलिसी नियुक्त करतो आणि टाइमस्टॅम्प, डिव्हाइस आयडेंटिफायर आणि वापरकर्ता आयडेंटिटीसह ऑथेंटिकेशन इव्हेंट लॉग करतो. जेव्हा ॲक्टिव्ह डिरेक्टरीमध्ये कर्मचाऱ्याचे खाते अक्षम केले जाते, तेव्हा त्यांचा वायरलेस ॲक्सेस पुढील री-ऑथेंटिकेशन सायकलवर रद्द केला जातो — साधारणपणे काही मिनिटांत.
IEEE 802.11ax (Wi-Fi 6) स्पेसिफिकेशनमध्ये सादर केलेले WPA3-Enterprise, संवेदनशील वातावरणासाठी 192-बिट सिक्युरिटी मोड अनिवार्य करून आणि सायमलटेनियस ऑथेंटिकेशन ऑफ इक्वल्स (SAE) हँडशेकद्वारे फॉरवर्ड सिक्रसी प्रदान करून याला अधिक मजबूत करते. नवीन डिप्लॉयमेंटसाठी, WPA3-Enterprise हे सर्व क्लिनिकल आणि ऑपरेशनल झोनसाठी बेसलाइन मानक असावे.
ट्रान्समिशन सिक्युरिटी आणि एन्क्रिप्शन मानके
HIPAA §164.312(e)(2)(ii) नुसार संस्थांनी योग्य वाटेल तेव्हा ट्रान्झिटमध्ये ePHI एन्क्रिप्ट करण्यासाठी यंत्रणा लागू करणे आवश्यक आहे. व्यवहारात, ePHI चे कोणतेही वायरलेस ट्रान्समिशन एन्क्रिप्ट केलेले असणे आवश्यक आहे. ॲप्लिकेशन-लेयर एन्क्रिप्शनसाठी किमान स्वीकार्य मानक TLS 1.2 आहे, नवीन डिप्लॉयमेंटसाठी TLS 1.3 ची जोरदार शिफारस केली जाते. वायरलेस लेयरवर, WPA3 जुन्या TKIP आणि AES-CCMP-128 मानकांना बदलून CCMP-256 (काउंटर मोड सायफर ব্লক चेनिंग मेसेज ऑथेंटिकेशन कोड प्रोटोकॉल) एन्क्रिप्शन प्रदान करते.
NHS संस्थांसाठी, HSCN (हेल्थ अँड सोशल केअर नेटवर्क) सेवांकडे ट्रान्झिटमधील डेटा HSCN सुरक्षा आवश्यकतांचे पालन करणे आवश्यक आहे, जे किमान TLS 1.2 अनिवार्य करतात आणि SSL 3.0, TLS 1.0 आणि TLS 1.1 च्या वापरास प्रतिबंधित करतात. HSCN-बाउंड ट्रॅफिक टर्मिनेट करणारा कोणताही वायरलेस ॲक्सेस पॉईंट किंवा कंट्रोलर या सायफर सूट निर्बंधांची अंमलबजावणी करण्यासाठी कॉन्फिगर केलेला असणे आवश्यक आहे.
IoMT डिव्हाइस मॅनेजमेंट: सर्वात कठीण समस्या
इंटरनेट ऑफ मेडिकल थिंग्ज हेल्थकेअर वायरलेस डिप्लॉयमेंटमध्ये सर्वात तांत्रिकदृष्ट्या गुंतागुंतीचे कंप्लायन्स आव्हान उभे करते. लेगसी वैद्यकीय उपकरणे — इन्फ्युजन पंप, पेशंट मॉनिटर्स, टेलिमेट्री सिस्टीम, इमेजिंग उपकरणे — वारंवार एम्बेडेड ऑपरेटिंग सिस्टीम चालवतात जे 802.1X ऑथेंटिकेशन किंवा आधुनिक TLS आवृत्त्यांना समर्थन देऊ शकत नाहीत. व्यवस्थापित एंडपॉइंट्सच्या समान वेळापत्रकानुसार त्यांना पॅच केले जाऊ शकत नाही आणि त्यांचे उत्पादक अनेकदा डिव्हाइस सर्टिफिकेशनवर परिणाम करणारे बदल करण्यास मनाई करतात.
कंप्लायंट दृष्टीकोन म्हणजे कठोर कम्युनिकेशन पाथ कंट्रोल्ससह एकत्रित मायक्रो-सेगमेंटेशन. प्रत्येक डिव्हाइस प्रकार किंवा डिव्हाइस फॅमिली एका समर्पित सब-VLAN ला नियुक्त केली जाते. फायरवॉल ACLs केवळ विशिष्ट सोर्स/डेस्टिनेशन IP पेअर्स, प्रोटोकॉल आणि पोर्ट्सना परवानगी देतात जे डिव्हाइसला त्याच्या क्लिनिकल कार्यासाठी आवश्यक असतात. इतर सर्व ट्रॅफिक ब्लॉक आणि लॉग केले जाते. नेटवर्क ॲक्सेस कंट्रोल (NAC) सोल्यूशन्स डिव्हाइस प्रोफाइलिंगची अंमलबजावणी करू शकतात — इन्फ्युजन पंप असल्याचा दावा करणारे डिव्हाइस नियुक्त केलेली पॉलिसी मंजूर होण्यापूर्वी खरोखरच तसे वागते याची खात्री करणे.
DSPT स्टँडर्ड 9 विशेषतः असमर्थित सिस्टीमना संबोधित करते: संस्थांनी सध्याच्या सुरक्षा मानकांवर अपडेट न करता येणाऱ्या सर्व सिस्टीमची इन्व्हेंटरी राखली पाहिजे आणि भरपाई देणारे कंट्रोल्स (compensating controls) लागू केले पाहिजेत. IoMT उपकरणांसाठी, भरपाई देणारा कंट्रोल म्हणजे वर्धित मॉनिटरिंगसह एकत्रित नेटवर्क आयसोलेशन.
रुग्ण आणि अभ्यागत WiFi: घर्षणाशिवाय कंप्लायन्स
रुग्ण आणि अभ्यागत guest WiFi ही क्लिनिकल अनुभवाची आवश्यकता आहे, पर्यायी सुविधा नाही. संशोधन सातत्याने दर्शविते की कनेक्टिव्हिटी ॲक्सेस रुग्णांची चिंता कमी करतो, दीर्घ ॲडमिशन दरम्यान कौटुंबिक संवाद सुधारतो आणि एकूण रुग्ण समाधान स्कोअरमध्ये योगदान देतो. क्लिनिकल नेटवर्कमध्ये रिस्क वेक्टर तयार न करता ही सेवा वितरित करणे हे कंप्लायन्स आव्हान आहे.
कंप्लायंट पेशंट WiFi डिप्लॉयमेंटसाठी तीन घटकांची आवश्यकता असते. प्रथम, संपूर्ण नेटवर्क आयसोलेशन: गेस्ट SSID ने अंतर्गत क्लिनिकल सिस्टीम, EHR प्लॅटफॉर्म किंवा प्रशासकीय नेटवर्ककडे कोणताही मार्ग नसलेल्या समर्पित गेटवेद्वारे थेट इंटरनेटवर ट्रॅफिक राउट करणे आवश्यक आहे. दुसरे, GDPR-कंप्लायंट डेटा हँडलिंग: Captive Portal वर कॅप्चर केलेला कोणताही डेटा — ईमेल पत्ते, डिव्हाइस आयडेंटिफायर्स, अटींची स्वीकृती — यूके GDPR (NHS संस्थांसाठी) किंवा HIPAA च्या किमान आवश्यक मानकांनुसार (यूएस हेल्थकेअरसाठी) हाताळला जाणे आवश्यक आहे. तिसरे, बँडविड्थ मॅनेजमेंट: क्वालिटी ऑफ सर्व्हिस (QoS) पॉलिसींनी हे सुनिश्चित केले पाहिजे की अभ्यागत ट्रॅफिक वायरलेस माध्यमाला सॅच्युरेट करू शकत नाही आणि क्लिनिकल ॲप्लिकेशन कार्यप्रदर्शन खराब करू शकत नाही.
Purple चा guest WiFi प्लॅटफॉर्म विशेषतः या युज केससाठी डिझाइन केलेला आहे. तो GDPR-कंप्लायंट संमती प्रवाहांसह कॉन्फिगरेबल Captive Portal, रुग्ण संवादासाठी फर्स्ट-पार्टी डेटा कॅप्चर आणि WiFi analytics प्रदान करतो जे ऑपरेशन्स टीम्सना अभ्यागतांच्या ड्वेल टाइम्स, पीक युसेज पीरियड्स आणि ॲक्सेस पॉईंट लोडची दृश्यमानता देतात — हे सर्व क्लिनिकल नेटवर्कमध्ये कोणताही डेटा मार्ग न बनवता. NHS ट्रस्टसाठी, DSPT पुरावे सबमिशनला समर्थन देण्यासाठी Purple च्या डेटा हँडलिंग पद्धती दस्तऐवजीकरण केल्या आहेत.
NHS-विशिष्ट आवश्यकता कव्हर करणाऱ्या तपशीलवार डिप्लॉयमेंट मार्गदर्शकासाठी, NHS Staff WiFi: How to Deploy Secure Wireless Networks in Healthcare पहा.
अंमलबजावणी मार्गदर्शक
टप्पा 1: डिस्कव्हरी आणि रिस्क असेसमेंट (आठवडे 1-3)
सर्वसमावेशक वायरलेस साइट सर्वेक्षण आणि डिव्हाइस इन्व्हेंटरीसह प्रारंभ करा. सध्या कार्यरत असलेल्या प्रत्येक SSID, नेटवर्कशी कनेक्ट होणारा प्रत्येक डिव्हाइस प्रकार आणि वायरलेस लेयरवरून जाणारा प्रत्येक डेटा फ्लो मॅप करा. लेगसी वैद्यकीय उपकरणांकडे विशेष लक्ष द्या — त्यांच्या ऑपरेटिंग सिस्टीम आवृत्त्या, ऑथेंटिकेशन क्षमता आणि उत्पादक समर्थन स्थिती कॅटलॉग करा. ही इन्व्हेंटरी तुमच्या DSPT एव्हिडन्स पॅक आणि तुमच्या HIPAA रिस्क ॲनालिसिस डॉक्युमेंटेशनचा पाया बनते.
तुमच्या टार्गेट कंप्लायन्स फ्रेमवर्कच्या विरुद्ध गॅप ॲनालिसिस करा. HIPAA साठी, तांत्रिक सुरक्षा उपाय चेकलिस्टच्या विरुद्ध वर्तमान कंट्रोल्स मॅप करा. DSPT साठी, NDG 10 मानकांच्या विरुद्ध पूर्व-मूल्यांकन पूर्ण करा. शेअर्ड PSKs वापरात असलेले प्रत्येक उदाहरण ओळखा, जेथे नेटवर्क सेगमेंटेशन अनुपस्थित किंवा अपूर्ण आहे आणि जेथे ऑडिट लॉगिंग पुरेसा तपशील कॅप्चर करत नाही.
टप्पा 2: आर्किटेक्चर डिझाइन (आठवडे 4-6)
वर वर्णन केलेल्या फोर-झोन सेगमेंटेशन मॉडेलची रचना करा. VLAN असाइनमेंट्स, फायरवॉल पॉलिसी नियम आणि इंटर-झोन ACLs परिभाषित करा. RADIUS इन्फ्रास्ट्रक्चर निर्दिष्ट करा — ऑन-प्रिमाइसेस (Microsoft NPS, FreeRADIUS) किंवा क्लाउड-होस्टेड (RADIUS-as-a-Service). सर्टिफिकेट लाइफसायकल मॅनेजमेंट आणि रिव्होकेशन प्रक्रियेसह सर्टिफिकेट-आधारित ऑथेंटिकेशनसाठी PKI स्ट्रक्चर डिझाइन करा.
गेस्ट WiFi झोनसाठी, Captive Portal प्लॅटफॉर्म निवडा आणि कॉन्फिगर करा. डेटा कॅप्चर फील्ड्स, संमतीची भाषा आणि डेटा रिटेन्शन पॉलिसी परिभाषित करा. पोर्टलची गोपनीयता नोटीस GDPR कलम 13 आवश्यकता (UK/EU डिप्लॉयमेंटसाठी) किंवा HIPAA च्या नोटीस ऑफ प्रायव्हसी प्रॅक्टिसेस आवश्यकता (US डिप्लॉयमेंटसाठी) पूर्ण करते याची खात्री करा.
टप्पा 3: डिप्लॉयमेंट आणि मायग्रेशन (आठवडे 7-12)
झोन क्रमाने डिप्लॉय करा: ऑपरेशनल आणि IoMT झोन प्रथम (क्लिनिकल ऑपरेशन्ससाठी सर्वात कमी धोका), नंतर कर्मचारी झोन, नंतर गेस्ट. प्रत्येक झोनसाठी, चाचणी उपकरणांमधून क्रॉस-झोन ट्रॅफिकचा प्रयत्न करून सेगमेंटेशन प्रमाणित करा — फायरवॉल ACLs अपेक्षित ट्रॅफिक ब्लॉक करत असल्याची पुष्टी करा. सर्टिफिकेट रिव्होकेशनची चाचणी करून ऑथेंटिकेशन प्रमाणित करा — ॲक्टिव्ह डिरेक्टरीमध्ये चाचणी खाते अक्षम करा आणि अपेक्षित री-ऑथेंटिकेशन विंडोमध्ये वायरलेस ॲक्सेस नाकारला गेल्याची पुष्टी करा.
फेज्ड रोलआउट वापरून कर्मचारी उपकरणांना 802.1X ऑथेंटिकेशनवर मायग्रेट करा. तुमच्या MDM (मोबाइल डिव्हाइस मॅनेजमेंट) प्लॅटफॉर्मद्वारे व्यवस्थापित एंडपॉइंट्सवर डिव्हाइस सर्टिफिकेट्स डिप्लॉय करा. BYOD उपकरणांसाठी, एक स्वतंत्र ऑनबोर्डिंग SSID लागू करा जे कर्मचारी झोनमध्ये ॲक्सेस देण्यापूर्वी वापरकर्त्यांना सर्टिफिकेट इन्स्टॉलेशनद्वारे मार्गदर्शन करते.
टप्पा 4: ऑडिट लॉगिंग आणि मॉनिटरिंग (सुरू असलेले)
तुमच्या SIEM (सिक्युरिटी इन्फॉर्मेशन अँड इव्हेंट मॅनेजमेंट) प्लॅटफॉर्मवर ऑथेंटिकेशन लॉग फॉरवर्ड करण्यासाठी तुमचा RADIUS सर्व्हर आणि वायरलेस कंट्रोलर कॉन्फिगर करा. लॉग कॅप्चर करत असल्याची खात्री करा: टाइमस्टॅम्प, वापरकर्ता आयडेंटिटी, डिव्हाइस MAC ॲड्रेस, SSID, VLAN असाइनमेंट, सेशन कालावधी आणि ट्रान्सफर केलेले बाइट्स. HIPAA कंप्लायन्ससाठी, किमान सहा वर्षे लॉग राखून ठेवा. DSPT साठी, लॉगचे नियमितपणे पुनरावलोकन केले जाते आणि पुनरावलोकन प्रक्रियेचे दस्तऐवजीकरण केले जाते याची खात्री करा.
विसंगत वर्तनासाठी स्वयंचलित अलर्टिंग लागू करा: व्यावसायिक वेळेबाहेर कनेक्ट होणारी उपकरणे, असामान्य डेटा व्हॉल्यूम, थ्रेशोल्ड ओलांडणारे अयशस्वी ऑथेंटिकेशन प्रयत्न आणि अनपेक्षित VLAN वर दिसणारी उपकरणे.
सर्वोत्तम पद्धती (Best Practices)
सर्व नवीन ॲक्सेस पॉईंट डिप्लॉयमेंटसाठी बेसलाइन मानक म्हणून WPA3-Enterprise चा अवलंब करा. WPA3 हे WPA2 च्या तुलनेत लक्षणीयरीत्या मजबूत एन्क्रिप्शन आणि फॉरवर्ड सिक्रसी प्रदान करते आणि Wi-Fi 6 आणि Wi-Fi 6E प्रमाणित उपकरणांसाठी आवश्यक आहे. लेगसी WPA2 डिप्लॉयमेंट्स परिभाषित कालमर्यादेत मायग्रेशनसाठी शेड्यूल केले जावे.
क्लिनिकल किंवा ऑपरेशनल नेटवर्कवर कधीही शेअर्ड PSKs वापरू नका. लेगसी उपकरणे 802.1X ला समर्थन देऊ शकत नसल्यास, कठोर फायरवॉल मायक्रो-सेगमेंटेशनसह एकत्रित करून, भरपाई देणारा कंट्रोल म्हणून MAC-आधारित ऑथेंटिकेशन लागू करा. तुमच्या रिस्क रजिस्टरमध्ये भरपाई देणाऱ्या कंट्रोलचे दस्तऐवजीकरण करा.
लहान NHS ट्रस्ट आणि GP प्रॅक्टिसेससाठी RADIUS-as-a-Service लागू करा ज्यांच्याकडे ऑन-प्रिमाइसेस RADIUS सर्व्हर चालवण्यासाठी इन्फ्रास्ट्रक्चरचा अभाव आहे. क्लाउड-होस्टेड RADIUS सिंगल पॉईंट ऑफ फेल्युअर रिस्क दूर करते आणि सर्टिफिकेट लाइफसायकल मॅनेजमेंट सुलभ करते.
सेगमेंटेशन बाउंड्रीजला लक्ष्य करून त्रैमासिक वायरलेस पेनिट्रेशन चाचण्या घ्या. विशेषतः VLAN हॉपिंग, रोग (rogue) ॲक्सेस पॉईंट डिटेक्शन आणि Captive Portal बायपास भेद्यतेची चाचणी करा. तुमच्या DSPT एव्हिडन्स पॅक किंवा HIPAA रिस्क ॲनालिसिसमध्ये निष्कर्ष आणि उपाययोजनांचे दस्तऐवजीकरण करा.
तुमच्या NAC प्लॅटफॉर्मसह एकत्रित लाइव्ह डिव्हाइस इन्व्हेंटरी राखून ठेवा. वायरलेस इस्टेटवरील प्रत्येक डिव्हाइसचा ज्ञात मालक, परिभाषित पॉलिसी आणि दस्तऐवजीकरण केलेली पुनरावलोकन तारीख असावी. अज्ञात उपकरणांनी स्वयंचलित अलर्ट ट्रिगर केला पाहिजे आणि तपासणी प्रलंबित असेपर्यंत क्वारंटाइन केले पाहिजे.
विविध क्षेत्रांमध्ये लागू होणाऱ्या व्यापक एंटरप्राइझ WiFi सुरक्षा तत्त्वांसाठी, Wi-Fi in Auto: The Complete 2026 Enterprise Guide मधील मार्गदर्शन हेल्थकेअर वातावरणासाठी थेट लागू होणाऱ्या अनेक आर्किटेक्चर पॅटर्नला कव्हर करते.
ट्रबलशूटिंग आणि रिस्क मिटिगेशन
सामान्य फेल्युअर मोड 1: VLAN लीकेज
सर्वात वारंवार होणारे सेगमेंटेशन अपयश म्हणजे ॲक्सेस लेयरवर VLAN मिसकॉन्फिगरेशन. सर्व VLAN पास करण्यासाठी चुकीच्या पद्धतीने कॉन्फिगर केलेला ट्रंक पोर्ट, किंवा अति-परवानगी देणाऱ्या डेस्टिनेशनसह फायरवॉल नियम, शांतपणे क्रॉस-झोन ट्रॅफिकला परवानगी देऊ शकतो. मिटिगेशन: प्रत्येक कॉन्फिगरेशन बदलानंतर ॲक्टिव्ह पेनिट्रेशन टेस्टिंगसह सेगमेंटेशन प्रमाणित करा. अनपेक्षित इंटर-VLAN मार्ग शोधण्यासाठी स्वयंचलित नेटवर्क स्कॅनिंग टूल्स वापरा.
सामान्य फेल्युअर मोड 2: सर्टिफिकेट एक्स्पायरीमुळे क्लिनिकल व्यत्यय
जेव्हा डिव्हाइस सर्टिफिकेट्स स्वयंचलित नूतनीकरणाशिवाय कालबाह्य होतात, तेव्हा क्लिनिकल उपकरणे वायरलेस ॲक्सेस गमावतात — संभाव्यतः शिफ्टच्या मध्यभागी. मिटिगेशन: किमान 30-दिवसांच्या नूतनीकरण विंडोसह तुमच्या MDM प्लॅटफॉर्मद्वारे स्वयंचलित सर्टिफिकेट नूतनीकरण लागू करा. 60 दिवसांच्या आत कालबाह्य होणाऱ्या सर्टिफिकेट्ससाठी अलर्टिंग कॉन्फिगर करा. कठोर ॲक्सेस लॉगिंगसह, आपत्कालीन क्लिनिकल डिव्हाइस ॲक्सेससाठी ब्रेक-ग्लास PSK राखून ठेवा.
सामान्य फेल्युअर मोड 3: iOS/Android वर Captive Portal बायपास
आधुनिक मोबाइल ऑपरेटिंग सिस्टीम Captive Network Assist (CNA) वापरतात — एक हलका ब्राउझर जो Captive Portal रीडायरेक्ट्स इंटरसेप्ट करतो. iOS किंवा Android CNA वर्तनातील बदल पोर्टल फ्लो खंडित करू शकतात. मिटिगेशन: प्रत्येक OS अपडेट सायकल नंतर वर्तमान iOS आणि Android आवृत्त्यांवर Captive Portal फ्लोची चाचणी करा. Purple सारखा प्लॅटफॉर्म वापरा जो OS आवृत्त्यांमध्ये पोर्टल सुसंगतता सक्रियपणे राखतो.
सामान्य फेल्युअर मोड 4: नेटवर्क बदलानंतर IoMT उपकरणे निकामी होणे
लेगसी वैद्यकीय उपकरणे नेटवर्क बदलांसाठी अत्यंत संवेदनशील असतात. VLAN रि-नंबरिंग, फायरवॉल पॉलिसी अपडेट किंवा DHCP स्कोप बदल डिव्हाइस कनेक्टिव्हिटी खंडित करू शकतो. मिटिगेशन: क्लिनिकल वेळेत IoMT VLAN साठी चेंज फ्रीझ विंडो राखून ठेवा. प्रोडक्शन डिप्लॉयमेंटपूर्वी प्रातिनिधिक डिव्हाइस प्रकारांच्या विरुद्ध लॅब वातावरणात सर्व बदलांची चाचणी करा. IoMT VLAN वर परिणाम करणाऱ्या कोणत्याही नेटवर्क बदलापूर्वी डिव्हाइस उत्पादकांच्या क्लिनिकल इंजिनिअरिंग टीम्सना सामावून घ्या.
सामान्य फेल्युअर मोड 5: अपुरे ऑडिट लॉग रिटेन्शन
HIPAA ला सहा वर्षांचे लॉग रिटेन्शन आवश्यक आहे. अनेक वायरलेस कंट्रोलर्स 30 किंवा 90-दिवसांच्या लॉग रिटेन्शनवर डीफॉल्ट असतात. मिटिगेशन: योग्य रिटेन्शन पॉलिसींसह केंद्रीकृत SIEM वर लॉग फॉरवर्ड करण्यासाठी सर्व वायरलेस इन्फ्रास्ट्रक्चर कॉन्फिगर करा. तुमच्या HIPAA रिस्क ॲनालिसिस किंवा DSPT सेल्फ-असेसमेंटचा भाग म्हणून दरवर्षी रिटेन्शन कॉन्फिगरेशन प्रमाणित करा.
ROI आणि बिझनेस इम्पॅक्ट
नॉन-कंप्लायन्सच्या खर्चाच्या तुलनेत मोजले असता कंप्लायंट हेल्थकेअर WiFi साठी बिझनेस केस सरळ आहे. हेल्थकेअर संस्थेतील एकाच HIPAA ब्रीचची सरासरी एकूण किंमत $10.9 दशलक्ष असते — ज्यामध्ये नियामक दंड, कायदेशीर शुल्क, उपाययोजना आणि प्रतिष्ठेचे नुकसान समाविष्ट आहे. DSPT अपयश ज्यामुळे NHS राष्ट्रीय सिस्टीमचा ॲक्सेस गमावला जातो, ते थेट रुग्णांच्या सुरक्षिततेच्या परिणामांसह, दिवस किंवा आठवड्यांसाठी क्लिनिकल ऑपरेशन्स थांबवू शकते.
रिस्क मिटिगेशनच्या पलीकडे, एक सु-आर्किटेक्ट केलेली वायरलेस इस्टेट मोजता येण्याजोगे ऑपरेशनल रिटर्न्स देते. क्लिनिकल कर्मचारी कनेक्टिव्हिटी वर्कअराउंड्सवर कमी वेळ घालवतात — 2023 च्या NHS डिजिटल सर्वेक्षणात असे आढळून आले की 67% क्लिनिकल कर्मचाऱ्यांनी खराब कनेक्टिव्हिटीला उत्पादकतेतील अडथळा म्हणून नमूद केले आहे. MDM द्वारे स्वयंचलित डिव्हाइस ऑनबोर्डिंग वायरलेस ॲक्सेस समस्यांसाठी IT सर्व्हिस डेस्क तिकिटे कमी करते. आणि एक कंप्लायंट, सु-व्यवस्थापित गेस्ट WiFi सेवा — Purple च्या WiFi Analytics सारख्या प्लॅटफॉर्मद्वारे वितरित केलेली — फर्स्ट-पार्टी पेशंट डेटा जनरेट करते जो कम्युनिकेशन्स, सॅटिस्फॅक्शन सर्व्हे आणि ऑपरेशनल प्लॅनिंगला समर्थन देऊ शकतो.
NHS ट्रस्टसाठी, यशस्वी DSPT सबमिशन NHS शेअर्ड बिझनेस सर्व्हिसेस फ्रेमवर्क आणि राष्ट्रीय खरेदी मार्गांचा ॲक्सेस देखील अनलॉक करते, ज्यामुळे भविष्यातील तंत्रज्ञान संपादनाची किंमत कमी होते. कंप्लायंट वायरलेस आर्किटेक्चरमधील गुंतवणूक संपूर्ण डिजिटल इस्टेटमध्ये लाभांश देते.
तुमच्या हेल्थकेअर वातावरणात अंमलबजावणी समर्थन आणि कंप्लायंट गेस्ट WiFi डिप्लॉयमेंटसाठी, Purple's Healthcare WiFi solutions एक्सप्लोर करा किंवा तपशीलवार NHS Staff WiFi deployment guide चे पुनरावलोकन करा.
Definições Principais
ePHI (Electronic Protected Health Information)
Qualquer informação de saúde individualmente identificável que seja criada, recebida, mantida ou transmitida em formato eletrónico. Ao abrigo da HIPAA, isto inclui nomes de doentes, datas de prestação de serviços, números de processos clínicos e quaisquer outros dados que possam ser utilizados para identificar um doente em relação ao seu estado de saúde ou cuidados recebidos.
As equipas de TI deparam-se com isto ao desenharem políticas de segmentação de rede e de tratamento de dados. Qualquer sistema ou caminho de rede que possa transportar ePHI — incluindo redes sem fios utilizadas por pessoal clínico — enquadra-se nos requisitos de Salvaguardas Técnicas da HIPAA.
DSPT (Data Security and Protection Toolkit)
Uma estrutura anual de autoavaliação obrigatória pelo NHS England para todas as organizações que acedem a dados de doentes do NHS ou se ligam a sistemas do NHS. Baseado nas dez Normas de Segurança de Dados do National Data Guardian (NDG), exige que as organizações demonstrem que os dados pessoais são tratados de forma segura e que existem controlos técnicos e organizacionais adequados.
Os NHS Trusts, consultórios de medicina geral (GP practices) e fornecedores terceiros com acesso aos sistemas do NHS devem submeter anualmente o DSPT. Para redes sem fios, as normas mais relevantes são a Norma 1 (controlo de acessos), a Norma 6 (processamento lícito) e a Norma 9 (gestão de sistemas não suportados).
802.1X
Uma norma IEEE para controlo de acesso à rede baseado em portas. Fornece uma estrutura de autenticação que exige que os dispositivos apresentem credenciais válidas (normalmente um certificado ou utilizador/palavra-passe) a um servidor RADIUS antes de lhes ser concedido acesso à rede. Em implementações sem fios, o 802.1X é utilizado com EAP (Extensible Authentication Protocol) para autenticar utilizadores e dispositivos individuais.
A alternativa para PSKs partilhadas em ambientes empresariais e de saúde. Quando a conta de um colaborador é desativada no Active Directory, o seu acesso sem fios autenticado por 802.1X é automaticamente revogado — fornecendo a rastreabilidade de controlo de acessos exigida tanto pela HIPAA como pelo DSPT.
WPA3-Enterprise
A atual certificação de segurança da Wi-Fi Alliance para redes sem fios empresariais, introduzida com o Wi-Fi 6 (802.11ax). Exige o modo de segurança de 192 bits utilizando encriptação GCMP-256 e HMAC-SHA-384 para autenticação, proporcionando uma proteção significativamente mais forte do que o WPA2-Enterprise. Também oferece confidencialidade de encaminhamento (forward secrecy), o que significa que o comprometimento de uma chave de longo prazo não expõe o tráfego de sessões passadas.
A norma de encriptação de referência para novas implementações sem fios na área da saúde. Necessária para equipamentos certificados para Wi-Fi 6 e Wi-Fi 6E. As implementações legadas de WPA2 devem ser planeadas para migração como parte do programa de renovação tecnológica da organização.
RADIUS (Remote Authentication Dial-In User Service)
Um protocolo de rede que fornece autenticação, autorização e contabilização (AAA) centralizadas para acesso à rede. Em implementações sem fios, o servidor RADIUS valida credenciais 802.1X, atribui VLAN e políticas com base na identidade do utilizador ou dispositivo, e regista cada evento de autenticação com uma marca temporal e identificador do dispositivo.
O componente de infraestrutura central para acesso sem fios baseado em identidade. Pode ser implementado localmente (Microsoft NPS, FreeRADIUS) ou como um serviço na nuvem (RADIUS-as-a-Service). O registo de autenticação RADIUS é uma fonte primária de evidência para controlos de auditoria da HIPAA e requisitos de rastreabilidade de acessos do DSPT.
IoMT (Internet of Medical Things)
O ecossistema de dispositivos médicos ligados que comunicam através de redes IP, incluindo bombas de infusão, monitores de doentes, sistemas de telemetria, equipamentos de imagiologia e sensores vestíveis. Os dispositivos IoMT normalmente executam sistemas operativos integrados com capacidades de segurança limitadas e ciclos de substituição longos, criando desafios específicos para a conformidade da rede de saúde.
O desafio de conformidade tecnicamente mais complexo em implementações sem fios na área da saúde. Os dispositivos IoMT frequentemente não suportam autenticação 802.1X ou versões modernas de TLS, exigindo controlos compensatórios como autenticação baseada em MAC, micro-segmentação e monitorização avançada. A Norma 9 do DSPT exige especificamente que os sistemas não suportados (o que inclui muitos dispositivos IoMT) sejam inventariados e geridos com controlos compensatórios documentados.
Network Segmentation / VLAN
A prática de dividir uma rede física em múltiplas redes lógicas (Virtual Local Area Networks, ou VLANs) que estão isoladas umas das outras na camada de rede. O tráfego entre VLANs é controlado por políticas de firewall e listas de controlo de acesso. Na saúde, a segmentação é utilizada para isolar o tráfego clínico, de convidados, IoMT e operacional em domínios de políticas separados.
O controlo técnico fundamental para a conformidade de WiFi na área da saúde. Tanto a HIPAA como o DSPT exigem que o acesso a dados sensíveis seja restrito a utilizadores e sistemas autorizados. A segmentação de rede impõe isto na camada de infraestrutura, garantindo que um dispositivo convidado no WiFi de visitantes não consiga encaminhar tráfego para sistemas clínicos, mesmo que os controlos da camada de aplicação falhem.
Captive Portal
Uma página web que interceta o pedido HTTP/HTTPS inicial de um utilizador quando este se liga a uma rede WiFi, exigindo que conclua uma ação (aceitar os termos de serviço, introduzir credenciais ou fornecer dados de contacto) antes de lhe ser concedido acesso total à rede. Na saúde, os Captive Portals são utilizados para gerir a adesão ao WiFi de doentes e visitantes, recolher consentimento em conformidade com o GDPR e aplicar políticas de utilização aceitável.
O principal componente voltado para o utilizador numa implementação de WiFi de convidados em conformidade. Um Captive Portal por si só não torna uma rede de convidados conforme — a rede subjacente deve ainda estar devidamente segmentada e isolada. No entanto, um portal bem configurado (como a plataforma da Purple) trata da gestão de consentimento do GDPR, minimização de dados e registo de auditoria para a camada de acesso de convidados.
HSCN (Health and Social Care Network)
O serviço de rede gerido do NHS que fornece conectividade entre organizações de saúde e assistência social e os sistemas nacionais do NHS. A HSCN substituiu a N3 em 2019 e fornece uma rede IP segura e gerida para aceder a serviços nacionais, incluindo o NHS Spine, NHSmail e sistemas de informação clínica. As organizações que se ligam à HSCN devem cumprir requisitos de segurança específicos.
Relevante para organizações do NHS cuja infraestrutura sem fios fornece acesso a sistemas ligados à HSCN. Os pontos de acesso ou controladores sem fios que terminam tráfego destinado a serviços HSCN devem ser configurados para aplicar os requisitos de segurança da HSCN, incluindo o mínimo de TLS 1.2 e conjuntos de cifras aprovados.
Exemplos Práticos
Um NHS Trust com 450 camas está a preparar a sua submissão anual do DSPT e identificou que a equipa clínica está atualmente a utilizar uma WPA2 PSK partilhada no SSID da equipa. O diretor de TI precisa de migrar para um acesso baseado em identidade sem interromper as operações clínicas. O parque tecnológico inclui 280 portáteis Windows geridos, 120 dispositivos iOS registados no Jamf e aproximadamente 60 dispositivos médicos legados (bombas de infusão e monitores de cabeceira) que não suportam 802.1X.
Faseie a migração em quatro fluxos de trabalho a decorrer em paralelo. Primeiro, implemente um serviço RADIUS alojado na nuvem (ou configure o Microsoft NPS nos controladores de domínio existentes) e integre-o com o Active Directory. Segundo, utilize o Jamf para enviar perfis EAP-TLS e certificados de dispositivo para todos os 120 dispositivos iOS — isto pode ser concluído de forma silenciosa, sem intervenção do utilizador. Terceiro, implemente certificados nos 280 portáteis Windows através de Política de Grupo, configurando o perfil sem fios para utilizar EAP-TLS com o novo servidor RADIUS. Execute em simultâneo o SSID PSK legado e o novo SSID 802.1X durante a janela de migração, utilizando um SSID de integração dedicado para dispositivos que necessitem de instalação manual de certificados. Quarto, coloque os 60 dispositivos médicos legados numa VLAN IoMT dedicada utilizando autenticação baseada em MAC como controlo de compensação, com ACLs de firewall a restringir cada tipo de dispositivo apenas aos caminhos de comunicação necessários. Documente a autenticação baseada em MAC como um controlo de compensação no registo de riscos do DSPT, com uma data de revisão associada ao programa de substituição de dispositivos. Assim que todos os dispositivos geridos estiverem migrados, desative o SSID PSK partilhado e documente a migração no pacote de evidências do DSPT.
Um sistema de saúde dos EUA que opera três hospitais comunitários precisa de implementar WiFi em conformidade para doentes e visitantes em todos os locais. Cada local tem entre 150 e 300 camas, com elevados volumes de visitantes em áreas de espera, clínicas de consulta externa e refeitórios. O CIO pretende utilizar o WiFi de convidados para recolher dados de contacto dos doentes para inquéritos de satisfação pós-visita, mas a equipa jurídica levantou preocupações de HIPAA sobre a recolha de dados numa rede de saúde.
Implemente um SSID de WiFi de convidados dedicado numa VLAN separada em cada local, com o tráfego encaminhado diretamente para a internet através de um gateway dedicado — sem caminho de encaminhamento para sistemas clínicos internos, plataformas EHR ou redes administrativas. Implemente uma plataforma de Captive Portal (como a Purple) que faça a gestão do fluxo de integração de utilizadores. O portal deve apresentar um aviso de privacidade claro que explique quais os dados recolhidos, como serão utilizados e como os utilizadores podem autoexcluir-se — isto satisfaz o requisito de Aviso de Práticas de Privacidade do HIPAA para qualquer recolha de dados. Crucialmente, os dados recolhidos no portal (endereço de email, identificador do dispositivo, carimbo de data/hora da ligação) não constituem ePHI porque não estão associados a qualquer informação de saúde — são simplesmente dados de contacto recolhidos de um visitante. Configure o portal para recolher apenas os dados mínimos necessários para o caso de utilização do inquérito de satisfação: endereço de email e nome opcional. Garanta que os dados são armazenados no ambiente de nuvem da plataforma de WiFi de convidados, e não em qualquer sistema ligado à rede clínica. Implemente políticas de QoS de largura de banda para limitar o tráfego de convidados a 10 Mbps por dispositivo e 100 Mbps agregados por local, evitando que a utilização dos visitantes afete o desempenho das aplicações clínicas. Documente a arquitetura de isolamento de rede e as práticas de tratamento de dados na análise de risco do HIPAA.
Um grupo hospitalar privado no Reino Unido está a implementar Wi-Fi 6E numa instalação recém-construída. O arquiteto de rede precisa de conceber o parque sem fios para suportar tanto a conformidade com o DSPT como a preparação para inspeções da CQC (Care Quality Commission), ao mesmo tempo que proporciona uma experiência premium de WiFi para doentes que apoie o modelo de pagamento privado do hospital.
Conceba uma arquitetura de quatro zonas conforme descrito na secção de Análise Técnica Detalhada, aproveitando a banda de 6 GHz do Wi-Fi 6E para as zonas clínica e IoMT (menos interferência, maior taxa de transferência) e as bandas de 5 GHz e 2.4 GHz para a cobertura de doentes/visitantes. Implemente WPA3-Enterprise nas zonas clínicas com autenticação EAP-TLS integrada com o Active Directory do hospital. Para a zona de WiFi de doentes, implemente um Captive Portal premium com integração de marca, autenticação baseada no número do quarto (permitindo ao hospital associar sessões de WiFi aos registos dos doentes para fins de faturação e comunicações, com consentimento explícito do GDPR) e pacotes de largura de banda por níveis. Implemente a plataforma de WiFi de convidados da Purple para gerir o Captive Portal, a gestão de consentimento em conformidade com o GDPR e a análise de dados. O painel de análise fornece à equipa de operações visibilidade em tempo real sobre a carga dos pontos de acesso, taxas de conectividade dos doentes e períodos de pico de utilização — dados que apoiam tanto o planeamento operacional como as evidências da CQC sobre a experiência do doente. Garanta que os dados de WiFi dos doentes são tratados ao abrigo de um acordo de processamento de dados em conformidade com o GDPR com o fornecedor da plataforma. Documente a arquitetura de rede, os controlos de segmentação e as práticas de tratamento de dados no pacote de evidências de autoavaliação do DSPT.
Perguntas de Prática
Q1. A equipa de segurança de TI do seu NHS Trust acabou de concluir um levantamento de local sem fios e descobriu que o departamento de radiologia está a utilizar um WPA2 PSK partilhado para todos os dispositivos sem fios no departamento, incluindo estações de trabalho Windows geridas e três estações de trabalho de imagiologia DICOM antigas a correr Windows 7 (fora de suporte). A submissão do DSPT deve ser feita em seis semanas. Qual é o seu plano de ação imediato e como documenta isto para o DSPT?
Dica: Considere que a Norma 9 do DSPT aborda especificamente sistemas não suportados. Tem dois problemas distintos aqui: o PSK partilhado (controlo de acesso) e o SO não suportado (gestão de sistemas). Estes requerem abordagens de remediação diferentes e entradas de evidência DSPT diferentes.
Ver resposta modelo
Ações imediatas: (1) Migrar as estações de trabalho Windows geridas para autenticação 802.1X utilizando certificados de domínio existentes — isto pode ser concluído dentro da janela de seis semanas via Group Policy. (2) Colocar as três estações de trabalho DICOM Windows 7 numa VLAN IoMT dedicada com autenticação baseada em MAC e ACLs de firewall estritas que permitam apenas tráfego DICOM para o servidor PACS. (3) Documentar os sistemas Windows 7 no registo de riscos do DSPT sob a Norma 9 como 'sistemas não suportados com controlos de compensação', especificando o isolamento de rede como o controlo de compensação e incluindo uma data de substituição planeada. (4) Desativar o SSID PSK partilhado assim que todos os dispositivos geridos forem migrados. Para o pacote de evidências do DSPT: fornecer o diagrama de arquitetura de rede que mostra a nova segmentação, os registos de autenticação RADIUS que mostram a autenticação de utilizadores nomeados para dispositivos geridos, a entrada no registo de riscos para os sistemas Windows 7 e a configuração de ACL da firewall para a VLAN IoMT. A principal perspetiva do DSPT é que a Norma 9 não exige a substituição imediata de sistemas não suportados — exige que sejam identificados, avaliados quanto ao risco e geridos com controlos de compensação documentados.
Q2. O CISO de um sistema de saúde dos EUA recebeu um pedido da equipa de marketing para utilizar os dados de WiFi de pacientes do hospital para enviar e-mails promocionais sobre novos serviços aos pacientes que se ligaram durante a sua visita. A equipa de marketing argumenta que os pacientes forneceram o seu endereço de e-mail ao ligarem-se ao WiFi de convidados, pelo que o consentimento já foi dado. Isto está em conformidade com a HIPAA? Que controlos precisam de estar implementados?
Dica: Considere a distinção entre os dados recolhidos no portal WiFi (dados de contacto) e o contexto em que foram recolhidos (uma instalação de saúde). Considere também se o endereço de e-mail, combinado com o facto de a pessoa estar num hospital, constitui ePHI.
Ver resposta modelo
Esta é uma questão complexa da HIPAA. Um endereço de e-mail recolhido num portal Captive Portal de convidados não é, por si só, ePHI. No entanto, combinar esse endereço de e-mail com o facto de o indivíduo estar presente numa instalação de saúde numa data específica pode constituir ePHI — porque revela que a pessoa recebeu ou procurou serviços de saúde. Este é o problema da 'visita à instalação' na HIPAA: o mero facto de estar num hospital é informação de saúde. Para que o caso de uso de marketing esteja em conformidade: (1) A linguagem de consentimento do Captive Portal deve indicar explicitamente que o endereço de e-mail será utilizado para comunicações de marketing sobre serviços hospitalares — a aceitação genérica dos 'termos de serviço' não é suficiente. (2) O consentimento deve ser separado da concessão de acesso ao WiFi — os pacientes devem poder aceder ao WiFi sem consentir em receber e-mails de marketing (opt-in, não opt-out). (3) O tratamento de dados deve ser documentado no Aviso de Privacidade da HIPAA. (4) Se os e-mails de marketing fizerem referência à visita ou aos serviços de saúde do paciente, poderá ser necessária uma autorização HIPAA (e não apenas consentimento). A arquitetura mais segura é tratar qualquer endereço de e-mail recolhido num portal WiFi de uma instalação de saúde como potencialmente ePHI e tratá-lo em conformidade — com um BAA com o fornecedor da plataforma WiFi e consentimento explícito de opt-in para uso de marketing.
Q3. É o arquiteto de rede de um novo hospital privado de 200 camas que está a ser construído no Reino Unido. O diretor clínico quer implementar uma 'enfermaria inteligente' com 45 dispositivos IoMT por enfermaria (bombas de infusão, monitores de sinais vitais, sistemas de chamada de enfermeiros e camas inteligentes), todos sem fios. A equipa de gestão de instalações também quer ligar sistemas de gestão de edifícios (BMS), CCTV e controlo de acessos à mesma infraestrutura sem fios para reduzir os custos de cablagem. Como projeta a infraestrutura sem fios para cumprir os requisitos do DSPT e, ao mesmo tempo, acomodar todos estes casos de uso?
Dica: Pense cuidadosamente no número de domínios de política distintos de que necessita. As camas inteligentes e os sistemas de chamada de enfermeiros têm perfis de segurança diferentes dos das bombas de infusão. O BMS e o CCTV têm perfis de risco diferentes dos dispositivos clínicos. Considere se a partilha de infraestrutura física (pontos de acesso) mantendo a separação lógica (VLANs) é suficiente, ou se alguns tipos de dispositivos requerem separação física.
Ver resposta modelo
Projete uma arquitetura de seis zonas para este ambiente: (1) Pessoal Clínico — WPA3-Enterprise, 802.1X, integração com Active Directory. (2) Pacientes e Visitantes — Captive Portal, apenas internet, em conformidade com o GDPR. (3) IoMT Crítico (bombas de infusão, monitores de sinais vitais) — VLAN dedicada, certificados de dispositivo onde suportado, ACLs estritas, monitorização melhorada, sem infraestrutura partilhada com zonas não clínicas. (4) IoMT Não Crítico (camas inteligentes, chamada de enfermeiros) — VLAN separada do IoMT crítico, ACLs menos restritivas mas ainda assim isoladas do pessoal clínico e das zonas de convidados. (5) Sistemas de Gestão de Edifícios — VLAN dedicada, fisicamente separada das zonas clínicas sempre que possível, sem encaminhamento para redes clínicas. (6) CCTV / Controlo de Acessos — VLAN dedicada, considere se esta deve estar numa rede fisicamente separada dada a sensibilidade de segurança dos dados de controlo de acessos. A principal consideração do DSPT é que os dados de CCTV e controlo de acessos são dados pessoais ao abrigo do GDPR do Reino Unido, e os dados do BMS podem ser dados operacionais sensíveis — estes não devem ser acessíveis a partir da zona de WiFi de pacientes ou de sistemas clínicos que tratam dados de pacientes. Para a zona de IoMT crítico, considere se a densidade de 45 dispositivos por enfermaria justifica pontos de acesso dedicados para essa zona em vez de APs partilhados com separação por VLAN — isto proporciona um isolamento físico mais forte e elimina o risco de configurações incorretas criarem caminhos entre zonas. Documente a arquitetura de zonas, a fundamentação de cada decisão de design e os controlos de compensação para quaisquer dispositivos que não suportem autenticação moderna no pacote de evidências do DSPT.
Continue a ler esta série
Compreender o Cisco SUDI: Identidade Ancorada em Hardware no Controlo de Acesso Seguro à Rede
Este guia explica como o Cisco SUDI fornece uma identidade criptograficamente segura e ancorada em hardware para a infraestrutura de rede empresarial. Saiba como substituir endereços MAC clonáveis por certificados 802.1AR imutáveis para proteger o controlo de acesso à rede do seu espaço.
How to Configure SCEP for Automated Enterprise WiFi Certificate Enrollment
Este guia explica como configurar o SCEP (Simple Certificate Enrollment Protocol) para a atribuição automatizada de certificados WiFi empresariais, cobrindo toda a arquitetura desde PKI e NDES até à implementação de perfis MDM e validação RADIUS. Destina-se a gestores de TI, arquitetos de rede e CTOs em hotéis, cadeias de retalho, estádios, centros de conferências e organizações do setor público que necessitam de ir além das chaves pré-partilhadas e implementar uma autenticação 802.1X EAP-TLS escalável e baseada em identidade. A plataforma de sobreposição na nuvem da Purple, independente de hardware, integra-se diretamente com esta arquitetura, fornecendo a camada de WiFi para convidados e BYOD que coexiste com a sua rede de colaboradores autenticada por certificado.
Como Implementar SCEP para a Inscrição Automatizada de Certificados WiFi
Este guia explica como implementar o SCEP (Simple Certificate Enrollment Protocol) para a inscrição automatizada de certificados WiFi em espaços empresariais. Abrange todo o plano de arquitetura - desde o design de PKI e integração de MDM até à sequência de implementação obrigatória de três passos - e mostra aos gestores de TI e arquitetos de rede como eliminar credenciais partilhadas, automatizar a gestão do ciclo de vida dos certificados e cumprir os requisitos de PCI DSS e GDPR à escala.