NHS Staff WiFi : Comment déployer des réseaux sans fil sécurisés dans le secteur de la santé
Ce guide de référence technique détaille l'architecture, les protocoles de sécurité et les stratégies de déploiement pour le NHS Staff WiFi, couvrant l'authentification 802.1X, la segmentation VLAN, les politiques BYOD et la conformité au DSP Toolkit. Il fournit des conseils pratiques aux responsables informatiques pour déployer des réseaux sans fil de classe entreprise destinés aux utilisateurs cliniques, administratifs et invités sur une infrastructure physique partagée, sans compromettre la sécurité. Que vous planifiez un nouveau déploiement ou que vous renforciez un parc existant, ce guide fournit les cadres de décision et les étapes de mise en œuvre nécessaires pour agir dès ce trimestre.
Écouter ce guide
Voir la transcription du podcast
📚 Fait partie de notre série principale : Enterprise WiFi Security Guide →

कार्यकारी सारांश
NHS संपत्तियों में सुरक्षित, विश्वसनीय WiFi तैनात करना अब कोई वैकल्पिक सुविधा नहीं है — यह एक महत्वपूर्ण नैदानिक बुनियादी ढांचा (clinical infrastructure) है। मोबाइल-फर्स्ट रोगी देखभाल, इलेक्ट्रॉनिक स्वास्थ्य रिकॉर्ड (EHR), और जुड़े हुए चिकित्सा उपकरणों की ओर बढ़ता झुकाव एक ऐसे वायरलेस आर्किटेक्चर की मांग करता है जो कड़े सुरक्षा नियंत्रणों के साथ निर्बाध रोमिंग को संतुलित करे।
IT प्रबंधकों, नेटवर्क आर्किटेक्ट्स और CTOs के लिए, मुख्य चुनौती सुरक्षा से समझौता किए बिना साझा भौतिक बुनियादी ढांचे पर विभिन्न उपयोगकर्ता समूहों — नैदानिक कर्मचारियों, प्रशासनिक कर्मियों, रोगियों और मेहमानों — को समायोजित करना है, जो NHS डेटा सुरक्षा और संरक्षण (DSP) टूलकिट आवश्यकताओं को पूरा करता हो। यह मार्गदर्शिका NHS स्टाफ WiFi के लिए तकनीकी आवश्यकताओं का विवरण देती है, जिसमें IEEE 802.1X जैसे मजबूत प्रमाणीकरण ढांचे, VLANs के माध्यम से तार्किक नेटवर्क विभाजन (logical network segmentation), और Bring Your Own Device (BYOD) एंडपॉइंट्स के सुरक्षित ऑनबोर्डिंग पर ध्यान केंद्रित किया गया है।
विरासत (legacy) प्री-शेयर्ड कीज़ (PSK) से दूर जाकर और पहचान-संचालित एक्सेस नीतियों को अपनाकर, स्वास्थ्य सेवा संगठन उल्लंघन के जोखिम को कम कर सकते हैं, परिचालन संबंधी बाधाओं को कम कर सकते हैं, और डिजिटल परिवर्तन कार्यक्रमों के लिए वायरलेस आधार प्रदान कर सकते हैं। इसका व्यावसायिक पक्ष भी उतना ही मजबूत है: हेल्पडेस्क ओवरहेड में कमी, प्रमाणित DSP टूलकिट अनुपालन, और एक ऐसा नेटवर्क जो बिना किसी पूर्ण बुनियादी ढांचे के पुनर्निर्माण के भविष्य के नैदानिक नवाचारों का समर्थन करने में सक्षम हो।
तकनीकी गहन विश्लेषण
प्रमाणीकरण और एक्सेस नियंत्रण
एक सुरक्षित स्वास्थ्य सेवा वायरलेस नेटवर्क की नींव पहचान-आधारित एक्सेस नियंत्रण है। प्री-शेयर्ड कीज़ का उपयोग करने वाले विरासत WPA2-Personal नेटवर्क नैदानिक वातावरण के लिए मौलिक रूप से अनुपयुक्त हैं। वे कोई व्यक्तिगत जवाबदेही प्रदान नहीं करते हैं, कर्मचारियों के जाने पर ऑनबोर्डिंग हटाने की प्रक्रिया को जटिल बनाते हैं, और क्रेडेंशियल के साथ समझौता होने या इच्छित समूह से बाहर साझा किए जाने पर विफलता का एक एकल बिंदु (single point of failure) पेश करते हैं।
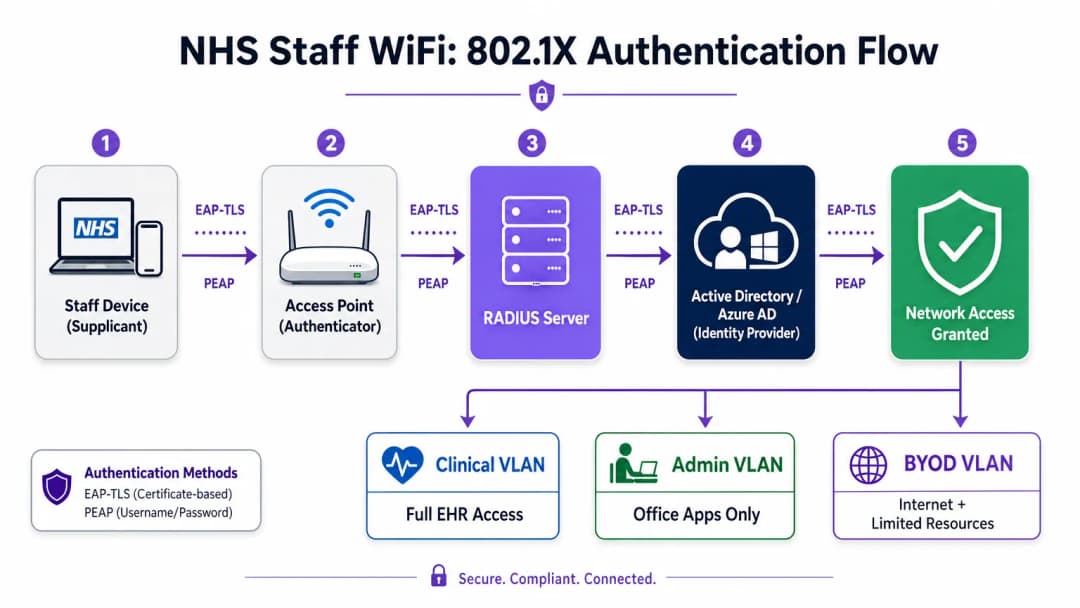
आधुनिक NHS तैनाती में WPA3-Enterprise (या न्यूनतम संक्रमण स्थिति के रूप में WPA2-Enterprise) को IEEE 802.1X प्रमाणीकरण का उपयोग करके अनिवार्य किया जाना चाहिए। इस ढांचे के लिए आवश्यक है कि नेटवर्क एक्सेस दिए जाने से पहले प्रत्येक उपयोगकर्ता या डिवाइस अद्वितीय क्रेडेंशियल प्रस्तुत करे, और उस प्रमाणीकरण का परिणाम यह निर्धारित करता है कि डिवाइस को किस तार्किक नेटवर्क सेगमेंट पर रखा जाए।
स्वास्थ्य सेवा तैनाती में दो EAP तरीके हावी हैं:
| EAP तरीका | प्रमाणीकरण तंत्र | इसके लिए सबसे उपयुक्त | सुरक्षा स्तर |
|---|---|---|---|
| EAP-TLS | क्लाइंट-साइड डिजिटल प्रमाणपत्र | कॉर्पोरेट-प्रबंधित नैदानिक उपकरण | उच्चतम — फ़िशिंग के लिए कोई पासवर्ड नहीं |
| PEAP-MSCHAPv2 | एन्क्रिप्टेड टनल में उपयोगकर्ता नाम/पासवर्ड | BYOD, व्यवस्थापक कर्मचारी, विरासत उपकरण | उच्च — TLS द्वारा सुरक्षित क्रेडेंशियल |
EAP-TLS कॉर्पोरेट उपकरणों के लिए स्वर्ण मानक (gold standard) है। प्रमाणपत्रों को मोबाइल डिवाइस मैनेजमेंट (MDM) प्लेटफॉर्म के माध्यम से वितरित किया जाता है, जिससे ज़ीरो-टच प्रमाणीकरण सक्षम होता है — डिवाइस पृष्ठभूमि में चुपचाप प्रमाणित हो जाता है। PEAP-MSCHAPv2 एक एन्क्रिप्टेड TLS सत्र के भीतर एक्टिव डायरेक्ट्री या एज़्योर AD क्रेडेंशियल को सुरक्षित रूप से टनल करता है, जिससे यह BYOD परिदृश्यों के लिए उपयुक्त हो जाता है जहां प्रमाणपत्र प्रबंधन व्यावहारिक नहीं है।
वायरलेस बुनियादी ढांचे को संगठन के केंद्रीय पहचान प्रदाता (IdP) के साथ एकीकृत करना यह सुनिश्चित करता है कि किसी कर्मचारी का AD खाता अक्षम होने पर एक्सेस स्वचालित रूप से रद्द हो जाए, जो सीधे एक्सेस लाइफसाइकल प्रबंधन के लिए DSP टूलकिट आवश्यकताओं को पूरा करता है।
नेटवर्क विभाजन और ट्रस्ट ज़ोन
भौतिक एक्सेस पॉइंट पूरे अस्पताल के फर्श पर प्रसारण करते हैं, लेकिन तार्किक विभाजन यह सुनिश्चित करता है कि न्यूनतम विशेषाधिकार के सिद्धांत के आधार पर ट्रैफ़िक अलग रहे। स्वास्थ्य सेवा सेटिंग में एक फ्लैट नेटवर्क आर्किटेक्चर एक गंभीर सुरक्षा भेद्यता है, जो एक समझौता किए गए अतिथि डिवाइस या कमजोर IoT सेंसर को संभावित रूप से नैदानिक प्रणालियों तक पहुँचने की अनुमति देता है।
सर्वोत्तम अभ्यास विशिष्ट SSIDs के लिए मैप किए गए अलग वर्चुअल लोकल एरिया नेटवर्क (VLANs) बनाने का निर्देश देता है, जिसमें फ़ायरवॉल नियम उनके बीच ट्रैफ़िक सीमाओं को लागू करते हैं:
| ज़ोन | SSID | प्रमाणीकरण | एक्सेस | QoS प्राथमिकता |
|---|---|---|---|---|
| नैदानिक | NHS-Clinical | EAP-TLS (प्रमाणपत्र) | EHR, PACS, नैदानिक संदेश सेवा | उच्चतम |
| प्रशासनिक | NHS-Staff | PEAP (AD क्रेडेंशियल) | ऑफिस ऐप्स, इंटरनेट | मध्यम |
| मेडिकल IoT | Hidden/MAB | MAC Authentication Bypass | केवल डिवाइस कंट्रोलर | उच्च |
| अतिथि / रोगी | NHS-Guest | Captive Portal | केवल इंटरनेट | निम्न |
| BYOD | NHS-BYOD | PEAP (AD क्रेडेंशियल) | इंटरनेट, सीमित VDI | निम्न |
मेडिकल IoT VLAN विशेष ध्यान देने योग्य है। कई जुड़े हुए चिकित्सा उपकरण — इन्फ्यूजन पंप, रोगी मॉनिटर, वायरलेस कॉल सिस्टम — 802.1X का समर्थन नहीं कर सकते हैं। MAC Authentication Bypass (MAB) इसका विकल्प है, लेकिन इसे सख्त फ़ायरवॉल एक्सेस कंट्रोल लिस्ट (ACLs) के साथ जोड़ा जाना चाहिए जो इन उपकरणों को केवल उनके निर्दिष्ट प्रबंधन सर्वर के साथ संचार करने तक सीमित करते हैं।
BYOD की चुनौती
Bring Your Own Device नीतियां प्रशासनिक कर्मचारियों और आने वाले चिकित्सकों के लिए तेजी से आम हो रही हैं। हालांकि, अप्रबंधित व्यक्तिगत उपकरण एक महत्वपूर्ण जोखिम का प्रतिनिधित्व करते हैं यदि उन्हें विश्वसनीय नेटवर्क सेगमेंट पर जाने की अनुमति दी जाती है।
एक सुरक्षित BYOD तैनाती में इन उपकरणों को एक समर्पित BYOD VLAN पर ऑनबोर्ड करना शामिल है। यह ज़ोन इंटरनेट एक्सेस प्रदान करता है और शायद एक सुरक्षित गेटवे या वर्चुअल डेस्कटॉप इंफ्रास्ट्रक्चर (VDI) के माध्यम से विशिष्ट, गैर-संवेदनशील आंतरिक संसाधनों तक सीमित पहुंच प्रदान करता है। इसमें नैदानिक प्रणालियों या रोगी डेटा स्टोर के लिए सीधे रूटिंग की अनुमति बिल्कुल नहीं होनी चाहिए।

कार्यान्वयन मार्गदर्शिका
एक सुरक्षित NHS स्टाफ WiFi आर्किटेक्चर को तैनात करने के लिए चल रहे नैदानिक संचालन में व्यवधान को कम करने के लिए चरणबद्ध दृष्टिकोण की आवश्यकता होती है।
चरण 1: मूल्यांकन और डिज़ाइन
एक व्यापक वायरलेस साइट सर्वेक्षण के साथ शुरुआत करें। लीड-लाइनेड दीवारों, भारी मशीनरी और घनी आबादी के कारण स्वास्थ्य सेवा वातावरण रेडियो फ्रीक्वेंसी (RF) प्रसार के लिए कुख्यात रूप से कठिन हैं। डिज़ाइन में केवल कवरेज ही नहीं, बल्कि क्षमता का भी ध्यान रखा जाना चाहिए, जिससे आपातकालीन विभागों और बाह्य रोगी क्लीनिकों जैसे उच्च-यातायात वाले क्षेत्रों में पर्याप्त एक्सेस पॉइंट घनत्व सुनिश्चित हो सके।
आवश्यक SSIDs को परिभाषित करें और उन्हें संबंधित VLANs और सुरक्षा नीतियों से मैप करें। प्रसारण SSIDs की संख्या को न्यूनतम रखें — आदर्श रूप से चार से अधिक नहीं — ताकि प्रबंधन ओवरहेड को कम किया जा सके और बीकन फ्रेम कंजेशन को कम किया जा सके, जो समग्र नेटवर्क प्रदर्शन को कम करता है।
चरण 2: बुनियादी ढांचा कॉन्फ़िगरेशन
परिभाषित VLANs का समर्थन करने के लिए कोर स्विचिंग और रूटिंग बुनियादी ढांचे को कॉन्फ़िगर करें। न्यूनतम विशेषाधिकार लागू करने के लिए सेगमेंट के बीच की सीमाओं पर फ़ायरवॉल नियम लागू करें। RADIUS सर्वर (जैसे, Cisco ISE, Aruba ClearPass, या क्लाउड-आधारित RADIUS-as-a-Service) सेट करें और इसे केंद्रीय पहचान प्रदाता के साथ एकीकृत करें। जिन वातावरणों में Purple का प्लेटफ़ॉर्म तैनात है, वहां इस चरण में WiFi Analytics को एकीकृत करना नेटवर्क उपयोग, रोमिंग पैटर्न और क्षमता हॉटस्पॉट में दृश्यता प्रदान करता है।
चरण 3: नीति प्रवर्तन और ऑनबोर्डिंग
प्रमाणीकरण नीतियां तैनात करें। कॉर्पोरेट उपकरणों के लिए, आवश्यक वायरलेस प्रोफाइल और क्लाइंट प्रमाणपत्र (EAP-TLS के लिए) भेजने के लिए MDM समाधान का उपयोग करें। यह सुनिश्चित करता है कि प्रबंधित उपकरण उपयोगकर्ता के हस्तक्षेप के बिना स्वचालित रूप से और सुरक्षित रूप से कनेक्ट हों।
BYOD के लिए, एक स्पष्ट ऑनबोर्डिंग वर्कफ़्लो स्थापित करें — आमतौर पर एक ऑनबोर्डिंग पोर्टल जो उपयोगकर्ता को उनके कॉर्पोरेट क्रेडेंशियल के साथ प्रमाणित करने, स्वीकार्य उपयोग नीति को स्वीकार करने और डिवाइस को सुरक्षित BYOD VLAN पर ले जाने के माध्यम से मार्गदर्शन करता है। Purple के Guest WiFi प्लेटफ़ॉर्म को रोगी और अतिथि SSID के लिए Captive Portal परत के रूप में तैनात किया जा सकता है, जो बड़े पैमाने पर GDPR-अनुरूप डेटा कैप्चर और शर्तों की स्वीकृति को संभालता है।
चरण 4: परीक्षण और सत्यापन
गो-लाइव से पहले, प्रत्येक प्रमाणीकरण पथ, VLAN असाइनमेंट और फ़ायरवॉल नियम का एंड-टू-एंड परीक्षण करें। विशेष रूप से पुनः प्रमाणीकरण घटनाओं की निगरानी करते हुए एक परीक्षण डिवाइस के साथ नैदानिक फर्श पर चलकर रोमिंग व्यवहार को मान्य करें। पुष्टि करें कि फास्ट रोमिंग प्रोटोकॉल (802.11r और 802.11k) सही ढंग से काम कर रहे हैं और एप्लिकेशन सत्र AP संक्रमणों के बाद भी बने रहते हैं।
सर्वोत्तम अभ्यास
प्री-शेयर्ड कीज़ को समाप्त करें। व्यक्तिगत जवाबदेही और केंद्रीकृत एक्सेस नियंत्रण सुनिश्चित करने के लिए सभी कर्मचारियों और नैदानिक नेटवर्क को 802.1X प्रमाणीकरण पर स्थानांतरित करें। यह DSP टूलकिट अनुपालन के लिए एक गैर-परक्राम्य आवश्यकता है।
सख्त विभाजन लागू करें। अतिथि, BYOD, या IoT ट्रैफ़िक को कभी भी नैदानिक डेटा के समान तार्किक सेगमेंट पर अनुमति न दें। डिफ़ॉल्ट नीति के रूप में स्पष्ट अस्वीकार (deny) नियमों के साथ, इंटर-VLAN रूटिंग को नियंत्रित करने के लिए स्टेटफुल फ़ायरवॉल का उपयोग करें।
नैदानिक ट्रैफ़िक को प्राथमिकता दें। विशेष रूप से उच्च भीड़ की अवधि के दौरान, अतिथि या प्रशासनिक ट्रैफ़िक की तुलना में नैदानिक अनुप्रयोगों — वॉयस ओवर WLAN, EHR एक्सेस — को प्राथमिकता देने के लिए वायरलेस कंट्रोलर और स्विच पर QoS नीतियां लागू करें।
फास्ट रोमिंग सक्षम करें। 802.11r (फास्ट BSS ट्रांज़िशन) और 802.11k (रेडियो रिसोर्स मेजरमेंट) को तैनात करें ताकि यह सुनिश्चित हो सके कि नैदानिक कर्मचारी एप्लिकेशन टाइमआउट या टूटे हुए कनेक्शन का अनुभव किए बिना सुविधा के माध्यम से आगे बढ़ सकें।
निरंतर निगरानी। नेटवर्क स्वास्थ्य की निगरानी करने, अनधिकृत एक्सेस पॉइंट की पहचान करने और उपयोगकर्ता रोमिंग व्यवहार को ट्रैक करने के लिए एनालिटिक्स प्लेटफॉर्म का उपयोग करें। फुटफॉल और उपयोग के पैटर्न को समझना — Retail और Hospitality वातावरण में सिद्ध एक तकनीक — क्षमता योजना और समस्या निवारण के लिए अस्पताल की सेटिंग में भी उतनी ही मूल्यवान है।
नियमित ऑडिटिंग। जहां लागू हो, DSP टूलकिट, साइबर एसेंशियल प्लस और ISO 27001 के साथ निरंतर अनुपालन सुनिश्चित करने के लिए वार्षिक वायरलेस जोखिम मूल्यांकन आयोजित करें।
समस्या निवारण और जोखिम शमन
प्रमाणीकरण टाइमआउट
उच्च क्लाइंट घनत्व वाले वातावरण में, RADIUS सर्वर अभिभूत हो सकते हैं, जिससे प्रमाणीकरण टाइमआउट और टूटे हुए कनेक्शन हो सकते हैं। सुनिश्चित करें कि RADIUS बुनियादी ढांचा पर्याप्त रूप से स्केल किया गया है और अत्यधिक उपलब्ध है। कई प्रमाणीकरण सर्वरों में लोड बैलेंसिंग लागू करें और एक प्रमुख परिचालन मीट्रिक के रूप में RADIUS प्रतिक्रिया समय की निगरानी करें।
रोमिंग के मुद्दे
वार्डों के बीच तेजी से चलने वाले नैदानिक कर्मचारियों को टूटे हुए कनेक्शन का अनुभव हो सकता है यदि वायरलेस बुनियादी ढांचा फास्ट रोमिंग प्रोटोकॉल का समर्थन नहीं करता है। वायरलेस कंट्रोलर पर 802.11r और 802.11k सक्षम करें और सुनिश्चित करें कि क्लाइंट डिवाइस इन मानकों का समर्थन करते हैं। कवरेज अंतराल या 'स्टिकी क्लाइंट' मुद्दों की पहचान करने और उन्हें हल करने के लिए पोस्ट-डिप्लॉयमेंट रोमिंग सर्वेक्षण आयोजित करें, जहां एक डिवाइस करीब जाने के बजाय दूर के, कमजोर AP से चिपका रहता है।
विरासत डिवाइस असंगतता
पुराने चिकित्सा उपकरण WPA3 या 802.1X जैसे आधुनिक सुरक्षा प्रोटोकॉल का समर्थन नहीं कर सकते हैं। MAB का उपयोग करके इन उपकरणों को एक समर्पित IoT VLAN पर अलग करें। उनके संचार को केवल आवश्यक प्रबंधन सर्वर तक सीमित करने के लिए सख्त फ़ायरवॉल नियम लागू करें। उन महत्वपूर्ण उपकरणों के लिए हार्डवेयर अपग्रेड या वायरलेस ब्रिज पर विचार करें जिन्हें मूल रूप से सुरक्षित नहीं किया जा सकता है।
प्रमाणपत्र की समाप्ति
EAP-TLS तैनाती परिभाषित समाप्ति अवधि वाले प्रमाणपत्रों पर निर्भर करती है। यदि प्रमाणपत्र नवीनीकरण के बिना समाप्त हो जाते हैं, तो डिवाइस प्रमाणित करने में विफल हो जाएंगे, जिससे व्यापक नैदानिक व्यवधान होगा। MDM प्लेटफॉर्म के माध्यम से SCEP (सिंपल सर्टिफिकेट एनरोलमेंट प्रोटोकॉल) के माध्यम से स्वचालित प्रमाणपत्र नवीनीकरण लागू करें, और सक्रिय रूप से प्रमाणपत्र समाप्ति तिथियों की निगरानी करें।
ROI और व्यावसायिक प्रभाव
एक सुरक्षित, एंटरप्राइज़-ग्रेड वायरलेस आर्किटेक्चर में निवेश नैदानिक, परिचालन और IT डोमेन में मापने योग्य रिटर्न प्रदान करता है।
नैदानिक दक्षता। विश्वसनीय कनेक्टिविटी यह सुनिश्चित करती है कि चिकित्सकों के पास देखभाल के बिंदु पर रोगी के रिकॉर्ड तक तत्काल पहुंच हो, जिससे जानकारी खोजने या टूटे हुए कनेक्शन से निपटने में लगने वाला समय कम हो जाता है। यह सीधे रोगी थ्रूपुट और देखभाल वितरण की गुणवत्ता को प्रभावित करता है।
कम IT ओवरहेड। साझा पासवर्ड और मैन्युअल ऑनबोर्डिंग से हटकर स्वचालित, प्रमाणपत्र-आधारित प्रमाणीकरण की ओर बढ़ने से पासवर्ड रीसेट और कनेक्टिविटी समस्याओं से संबंधित हेल्पडेस्क टिकटों में काफी कमी आती है। एक NHS ट्रस्ट ने 802.1X पर माइग्रेशन के बाद वायरलेस से संबंधित हेल्पडेस्क कॉल में 40% की कमी दर्ज की।
जोखिम शमन। सख्त विभाजन और मजबूत प्रमाणीकरण DSP टूलकिट आवश्यकताओं को पूरा करने, डेटा उल्लंघनों या अनुपालन विफलताओं से जुड़े वित्तीय और प्रतिष्ठित जोखिमों को कम करने के लिए मौलिक हैं। डेटा उल्लंघन की लागत उचित रूप से तैयार की गई वायरलेस संपत्ति में निवेश से कहीं अधिक है।
भविष्य के लिए तैयार करना (Future-Proofing)। एक अच्छी तरह से डिज़ाइन किया गया वायरलेस नेटवर्क भविष्य की डिजिटल स्वास्थ्य पहलों — स्थान-आधारित सेवाएं, रीयल-टाइम एसेट ट्रैकिंग, उन्नत टेलीहेल्थ एप्लिकेशन — के लिए आधार प्रदान करता है, जो Healthcare और Transport जैसे संबंधित क्षेत्रों में व्यापक रणनीतिक लक्ष्यों के साथ संरेखित होता है जहां मोबाइल कनेक्टिविटी परिचालन दक्षता को रेखांकित करती है।
उन संगठनों के लिए जो यह समझना चाहते हैं कि Purple का प्लेटफ़ॉर्म इस आर्किटेक्चर के अतिथि और रोगी WiFi परत से कैसे मेल खाता है, Healthcare उद्योग पृष्ठ NHS-संगत Captive Portal, एनालिटिक्स और GDPR-अनुरूप डेटा हैंडलिंग क्षमताओं का एक विस्तृत अवलोकन प्रदान करता है। वही एनालिटिक्स सिद्धांत जो Retail में ग्राहक जुड़ाव को बढ़ावा देते हैं, सीधे अस्पताल संपदा टीमों के लिए परिचालन खुफिया में अनुवादित होते हैं।
Définitions clés
IEEE 802.1X
Une norme IEEE pour le contrôle d'accès réseau basé sur les ports (PNAC). Elle fournit un mécanisme d'authentification aux appareils souhaitant se connecter à un LAN ou un WLAN, exigeant que chaque appareil présente des identifiants avant de se voir accorder l'accès.
Il s'agit de la norme obligatoire pour remplacer les mots de passe partagés non sécurisés par des connexions individuelles basées sur l'identité pour le personnel et les appareils cliniques. C'est la pierre angulaire d'une architecture sans fil conforme au DSP Toolkit.
VLAN (Virtual Local Area Network)
Un sous-réseau logique qui regroupe un ensemble d'appareils provenant de différents segments de réseau physique. Les VLANs permettent aux administrateurs réseau de partitionner un réseau commuté unique pour répondre aux exigences fonctionnelles et de sécurité de différents groupes d'utilisateurs.
Les VLANs sont essentiels pour segmenter le trafic clinique du trafic invité et administratif, limitant ainsi la zone d'impact d'une faille de sécurité potentielle et appliquant le principe du moindre privilège.
RADIUS (Remote Authentication Dial-In User Service)
Un protocole réseau qui fournit une gestion centralisée de l'authentification, de l'autorisation et de la comptabilité (AAA) pour les utilisateurs qui se connectent et utilisent un service réseau.
Le serveur RADIUS agit comme le moteur de décision entre les points d'accès sans fil et la base de données d'identité centrale (Active Directory), décidant qui obtient l'accès et à quel VLAN il est affecté.
EAP-TLS (Extensible Authentication Protocol - Transport Layer Security)
Une méthode EAP qui s'appuie sur des certificats client et serveur pour établir une connexion sécurisée et mutuellement authentifiée. Aucune des parties ne fait confiance à l'autre sans un certificat valide.
La méthode la plus sécurisée pour authentifier les appareils appartenant à l'hôpital. Les certificats distribués via MDM garantissent que seuls les terminaux gérés et de confiance peuvent accéder au réseau clinique, sans aucun mot de passe à hameçonner ou à partager.
MAB (MAC Authentication Bypass)
Une méthode d'authentification des appareils basée sur leur adresse MAC matérielle, utilisée comme solution de secours pour les appareils qui ne prennent pas en charge le 802.1X.
Nécessaire pour les appareils IoT médicaux existants qui ont besoin d'un accès réseau mais ne peuvent pas gérer des protocoles d'authentification complexes. Doit toujours être associé à des ACL de pare-feu strictes pour limiter l'appareil à ses chemins de communication autorisés.
DSP Toolkit (Data Security and Protection Toolkit)
Un outil d'auto-évaluation en ligne imposé par l'NHS England que toutes les organisations doivent remplir si elles ont accès aux données et aux systèmes des patients de l'NHS. Il s'aligne sur les dix normes de sécurité des données du National Data Guardian.
La conformité au DSP Toolkit est obligatoire pour les organisations de l'NHS et leurs fournisseurs. Une sécurité sans fil robuste — comprenant le 802.1X, la segmentation et la gestion du cycle de vie des accès — est un élément essentiel pour démontrer cette conformité.
SSID (Service Set Identifier)
Le nom principal associé à un réseau local sans fil 802.11, diffusé par les points d'accès pour permettre aux appareils clients de s'identifier et de se connecter au réseau.
Les hôpitaux doivent minimiser le nombre de SSIDs diffusés (par exemple, NHS-Clinical, NHS-Guest) afin de réduire la charge de gestion et la surcharge RF. Chaque SSID doit correspondre à une politique de sécurité et à un VLAN spécifiques.
QoS (Quality of Service)
Technologies qui gèrent le trafic de données pour réduire la perte de paquets, la latence et la gigue sur un réseau en priorisant certains types de trafic par rapport à d'autres.
Crucial dans le secteur de la santé pour garantir que les applications cliniques critiques et les communications vocales soient toujours prioritaires sur les trafics moins importants, tels que le streaming vidéo des invités ou les mises à jour logicielles.
802.11r (Fast BSS Transition)
Un amendement IEEE qui permet une itinérance rapide entre les points d'accès en pré-authentifiant le client auprès du point d'accès cible avant que la transition physique ne se produise, réduisant ainsi considérablement la latence d'itinérance.
Essentiel pour les environnements cliniques où le personnel est constamment en mouvement. Sans le 802.11r, les appareils doivent effectuer une réauthentification RADIUS complète à chaque changement de point d'accès, ce qui peut entraîner l'expiration des sessions d'application.
Exemples concrets
Un Trust de l'NHS déploie de nouveaux postes de travail mobiles (Workstations on Wheels) dans plusieurs services. L'équipe informatique doit s'assurer que ces appareils maintiennent leur connectivité lorsque le personnel infirmier se déplace entre les points d'accès, tout en garantissant que seuls les appareils autorisés peuvent accéder au VLAN clinique contenant le système de dossier de santé électronique.
Le Trust devrait mettre en œuvre un cadre d'authentification 802.1X utilisant EAP-TLS. L'équipe informatique utilisera sa solution MDM pour pousser un certificat client unique et le profil sans fil correspondant sur chaque poste de travail. Les contrôleurs sans fil seront configurés pour authentifier ces appareils auprès d'un serveur RADIUS, qui vérifie le certificat par rapport à la PKI interne. Une fois l'authentification réussie, le serveur RADIUS attribue dynamiquement le poste de travail au VLAN clinique dédié via un attribut RADIUS (par exemple, Tunnel-Private-Group-ID). Pour répondre au besoin d'itinérance, les protocoles 802.11r (Fast BSS Transition) et 802.11k (Radio Resource Measurement) doivent être activés sur l'infrastructure sans fil afin de permettre aux postes de travail de passer de manière transparente d'un point d'accès à un autre sans avoir à effectuer un cycle complet de réauthentification auprès du serveur RADIUS à chaque fois.
Un hôpital doit fournir un accès Internet aux médecins remplaçants de passage utilisant leurs ordinateurs portables personnels (BYOD). Ces médecins doivent accéder à des outils de référence médicale basés sur le cloud, mais il doit leur être strictement interdit d'accéder aux bases de données internes des patients de l'hôpital.
L'hôpital devrait déployer un SSID BYOD dédié, associé à un VLAN BYOD isolé. L'authentification doit être gérée via 802.1X en utilisant PEAP-MSCHAPv2, permettant aux remplaçants de se connecter à l'aide d'identifiants Active Directory temporaires fournis par les RH à leur arrivée. Le pare-feu central doit être configuré avec une ACL qui refuse explicitement tout routage du VLAN BYOD vers les VLAN cliniques ou administratifs, en autorisant uniquement le trafic sortant vers Internet. De plus, un Captive Portal peut être utilisé lors de la connexion initiale pour imposer une politique d'utilisation acceptable avant d'accorder un accès complet à Internet. Lorsque le compte AD temporaire du remplaçant est désactivé à la fin de sa mission, son accès sans fil est automatiquement révoqué.
Questions d'entraînement
Q1. Une nouvelle aile est ajoutée à l'hôpital et l'équipe des installations souhaite déployer des capteurs de température sans fil dans les réfrigérateurs de stockage des médicaments. Ces capteurs ne prennent en charge que le WPA2-Personal (clé pré-partagée) et ne peuvent pas utiliser le 802.1X. Comment l'architecte réseau doit-il les intégrer de manière sécurisée ?
Conseil : Considérez le principe du moindre privilège et la manière d'isoler les appareils non conformes des systèmes cliniques.
Voir la réponse type
L'architecte doit créer un SSID dédié et masqué, mappé sur un VLAN spécifique "Facilities IoT". Les capteurs se connecteront à l'aide de la PSK. De plus, des ACL de pare-feu strictes doivent être appliquées à ce VLAN, permettant aux capteurs de communiquer uniquement avec leur serveur de gestion central spécifique et refusant tout autre trafic — en particulier le routage vers le VLAN clinique ou Internet. Le MAC Authentication Bypass (MAB) doit également être configuré pour garantir que seules les adresses MAC spécifiques des capteurs achetés sont autorisées sur ce VLAN, empêchant ainsi les appareils non autorisés de se connecter en utilisant la même PSK.
Q2. Lors d'une garde matinale chargée, les infirmières signalent que leurs tablettes perdent fréquemment la connexion au système EHR lorsqu'elles parcourent le service, ce qui les oblige à se reconnecter. L'étude de couverture sans fil montre une force de signal élevée dans tout le service. Quelle est la cause probable et la solution ?
Conseil : Un signal fort ne garantit pas des transitions fluides entre les points d'accès. Considérez la surcharge d'authentification à chaque transition de point d'accès.
Voir la réponse type
La cause probable est l'absence de protocoles d'itinérance rapide. Lorsque la tablette s'éloigne de la zone de couverture d'un point d'accès et se connecte au suivant, elle est contrainte d'effectuer une réauthentification 802.1X complète auprès du serveur RADIUS, ce qui introduit une latence suffisante pour provoquer l'expiration de la session de l'application EHR. La solution consiste à activer le protocole 802.11r (Fast BSS Transition) sur les contrôleurs sans fil, ce qui permet au client de basculer en toute sécurité entre les points d'accès sans la latence d'un cycle de réauthentification complet. Le protocole 802.11k doit également être activé pour aider l'appareil à identifier le point d'accès cible optimal avant que la transition ne se produise.
Q3. Un Trust de l'NHS prépare son évaluation annuelle du DSP Toolkit. L'auditeur note que le personnel administratif utilise un mot de passe partagé pour accéder au réseau WiFi du personnel. Quel est le principal risque identifié ici et quelle est la correction recommandée ?
Conseil : Concentrez-vous sur la responsabilité individuelle et le cycle de vie des accès lorsque le personnel quitte l'organisation.
Voir la réponse type
Le principal risque est un manque de responsabilité individuelle et une mauvaise gestion du cycle de vie des accès. Si un membre du personnel administratif quitte le Trust, le mot de passe partagé reste valide, ce qui permet potentiellement un accès non autorisé. De plus, il est impossible d'auditer quel utilisateur spécifique a effectué une action sur le réseau. La solution consiste à abandonner le réseau à mot de passe partagé (PSK) et à migrer le personnel administratif vers un réseau authentifié 802.1X utilisant PEAP-MSCHAPv2 avec leurs identifiants Active Directory. Cela garantit la responsabilité individuelle et la révocation automatique des accès lorsque leur compte AD est désactivé lors de leur départ, répondant ainsi directement aux exigences du DSP Toolkit en matière de contrôle d'accès et de journaux d'audit.
Continuer la lecture de cette série
Comprendre Cisco SUDI : L'identité ancrée dans le matériel pour le contrôle d'accès réseau sécurisé
Ce guide explique comment Cisco SUDI fournit une identité sécurisée par cryptographie et ancrée dans le matériel pour l'infrastructure réseau d'entreprise. Découvrez comment remplacer les adresses MAC falsifiables par des certificats 802.1AR immuables afin de sécuriser le contrôle d'accès réseau de votre site.
Comment configurer SCEP pour l'enrôlement automatisé de certificats WiFi d'entreprise
Ce guide explique comment configurer SCEP (Simple Certificate Enrollment Protocol) pour l'enrôlement automatisé de certificats WiFi d'entreprise, couvrant l'architecture complète depuis la PKI et le NDES jusqu'au déploiement de profils MDM et à la validation RADIUS. Il s'adresse aux responsables informatiques, architectes réseau et CTO d'hôtels, de chaînes de vente au détail, de stades, de centres de conférence et d'organisations du secteur public qui souhaitent dépasser les clés pré-partagées et mettre en œuvre une authentification 802.1X EAP-TLS évolutive et basée sur l'identité. La plateforme cloud overlay de Purple, indépendante du matériel, s'intègre directement à cette architecture, fournissant la couche WiFi pour les invités et le BYOD qui coexiste avec votre réseau d'employés authentifié par certificat.
Comment implémenter SCEP pour l'enrôlement automatisé de certificats WiFi
Ce guide explique comment implémenter SCEP (Simple Certificate Enrollment Protocol) pour l'enrôlement automatisé de certificats WiFi dans les établissements d'entreprise. Il couvre l'ensemble du schéma architectural - de la conception de la PKI et l'intégration MDM à la séquence de déploiement obligatoire en trois étapes - et montre aux responsables informatiques et architectes réseau comment éliminer les identifiants partagés, automatiser la gestion du cycle de vie des certificats et respecter les exigences PCI DSS et GDPR à grande échelle.