WiFi 如何改善医院患者体验
本权威技术指南阐述了医院如何利用企业级访客 WiFi 基础设施和分析,以可衡量的方式改善住院体验。内容涵盖网络架构、合规要求(HIPAA、DSPT、GDPR)、Captive Portal 设计、导航集成和 ROI 框架,为 IT 决策者提供构建有力内部商业案例并成功部署的工具。
收听本指南
查看播客转录

Executive Summary
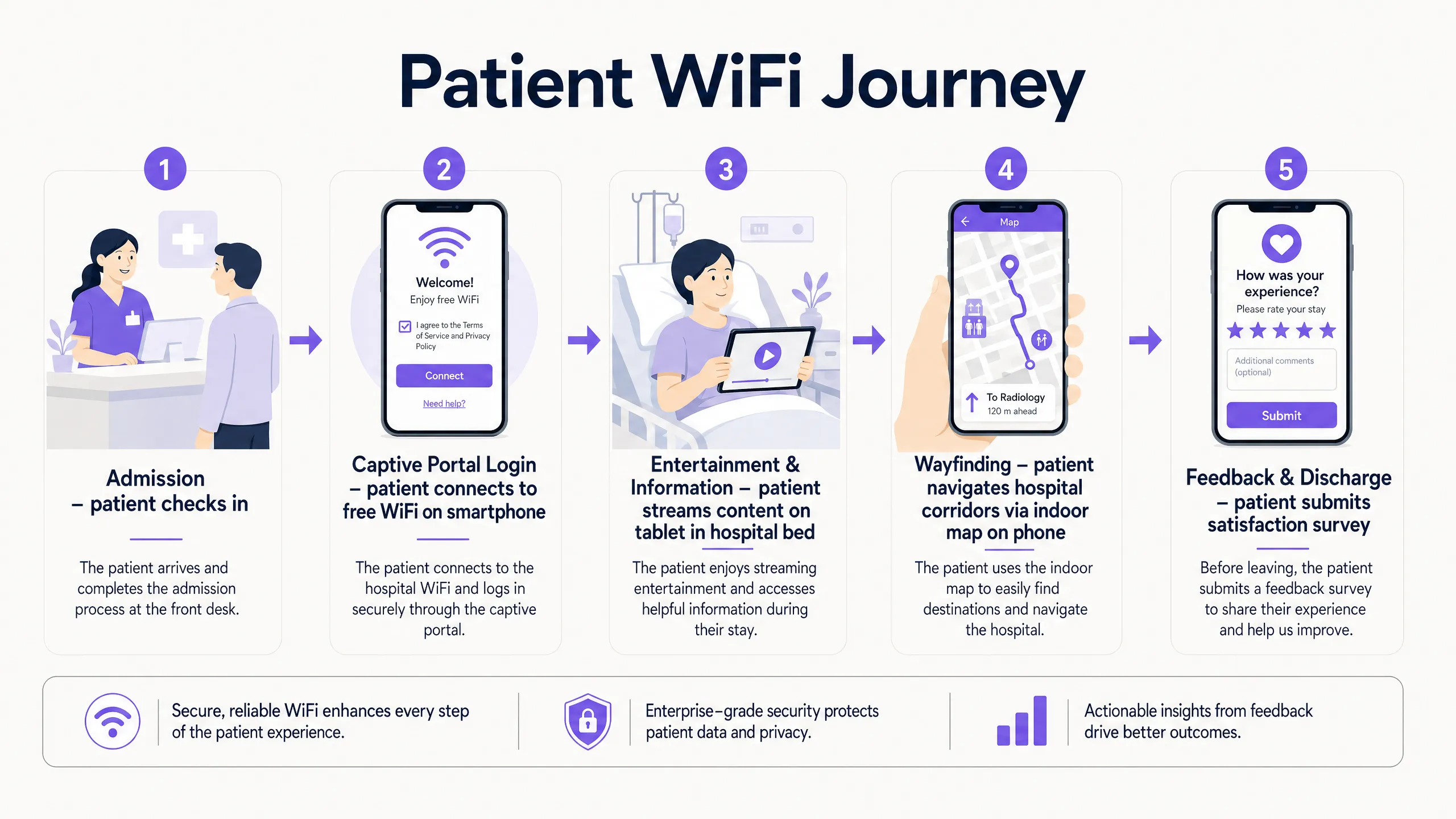
For modern healthcare facilities, free WiFi in hospitals has evolved from a basic amenity into a critical layer of patient experience and operational infrastructure. As hospitals digitise patient records, introduce telemedicine, and rely on connected medical devices, the underlying network architecture must simultaneously support clinical demands and rising patient expectations. This guide is for IT directors, network architects, and operations leaders who need to architect, deploy, and optimise a Guest WiFi solution that delivers measurable improvements to the inpatient experience — from entertainment and wayfinding to real-time feedback collection.
The core argument is straightforward: a well-deployed patient WiFi network, integrated with a WiFi Analytics platform, transforms the network from a passive utility into an active intelligence layer. It reduces missed appointments through indoor navigation, improves HCAHPS satisfaction scores through automated feedback, and gives operations teams the footfall data they need to optimise staffing and resource allocation. This guide covers the architecture, compliance requirements, implementation steps, and ROI framework to make that case internally and execute it successfully.
Technical Deep-Dive
Network Architecture for Healthcare Environments
Deploying enterprise-grade Guest WiFi in a hospital requires a fundamentally different approach to a standard commercial deployment. The primary constraint is the co-existence of clinical and guest traffic on the same physical infrastructure, which demands strict logical separation. The standard architecture uses 802.1Q VLANs to segment traffic into at minimum three tiers: clinical systems (EHR, PACS, telemetry), staff administrative networks, and the patient/visitor guest SSID.
The guest VLAN must be routed directly to a dedicated internet uplink — ideally a separate leased line — with no routing path to clinical VLANs. Firewall ACLs should enforce this at the distribution layer, not just at the perimeter. This is a non-negotiable architectural requirement under both HIPAA and the NHS DSPT framework. For a detailed breakdown of compliance obligations, refer to Healthcare WiFi: HIPAA, DSPT and WiFi Compliance Explained .
Access Point placement in hospitals presents unique RF challenges. Lead-lined radiology suites, reinforced concrete floors between wards, and high-density patient room clusters all create attenuation profiles that differ significantly from office environments. The design target for patient areas should be a minimum RSSI of -67 dBm with at least 20 dB signal-to-noise ratio. Critically, design for capacity, not just coverage. A ward with 30 beds may have 60-90 active devices at peak visiting hours — each potentially streaming video. AP selection should target devices supporting Wi-Fi 6 (802.11ax) or Wi-Fi 6E to handle that density efficiently.
Spectrum management is equally important. The 2.4 GHz band is heavily contested in hospital environments by legacy telemetry equipment, nurse call systems, and Bluetooth devices. Band steering should be configured to push capable devices to 5 GHz or 6 GHz bands. Automatic channel selection algorithms should be reviewed manually after deployment — they rarely produce optimal results in high-interference healthcare environments.
Captive Portal Architecture and Identity Management
The captive portal is the patient's first interaction with the hospital's digital services layer. It must be fast, reliable, and accessible across a wide range of devices — from the latest iPhone to a five-year-old Android tablet running a legacy browser. A poorly designed portal that fails to redirect correctly on certain devices will generate immediate complaints and support tickets.
Modern deployments move away from pre-shared keys entirely. The recommended approach is a social login or email-based captive portal that presents the hospital's terms of service and privacy notice, collects explicit consent for marketing communications (separately from network access consent, per GDPR Article 7), and authenticates the session. This flow, when integrated with a platform like Purple's Guest WiFi solution, simultaneously onboards the patient into a CRM-compatible data layer, enabling post-discharge communications and feedback surveys.
DNS-level security filtering should be applied to all guest traffic at the resolver level. This prevents access to known malicious domains, blocks inappropriate content categories, and provides an audit trail for compliance purposes. See Protect Your Network with Strong DNS and Security for implementation guidance on DNS filtering in guest network contexts.
WPA3-SAE (Simultaneous Authentication of Equals) should be the target encryption standard for any new SSID deployment. For legacy device compatibility, a WPA2/WPA3 transition mode is acceptable in the short term, but a migration timeline to WPA3-only should be planned. Client Isolation must be enabled on the guest SSID — this prevents device-to-device communication on the same network segment, which is critical for both security and GDPR compliance.
WiFi Analytics and Location Intelligence
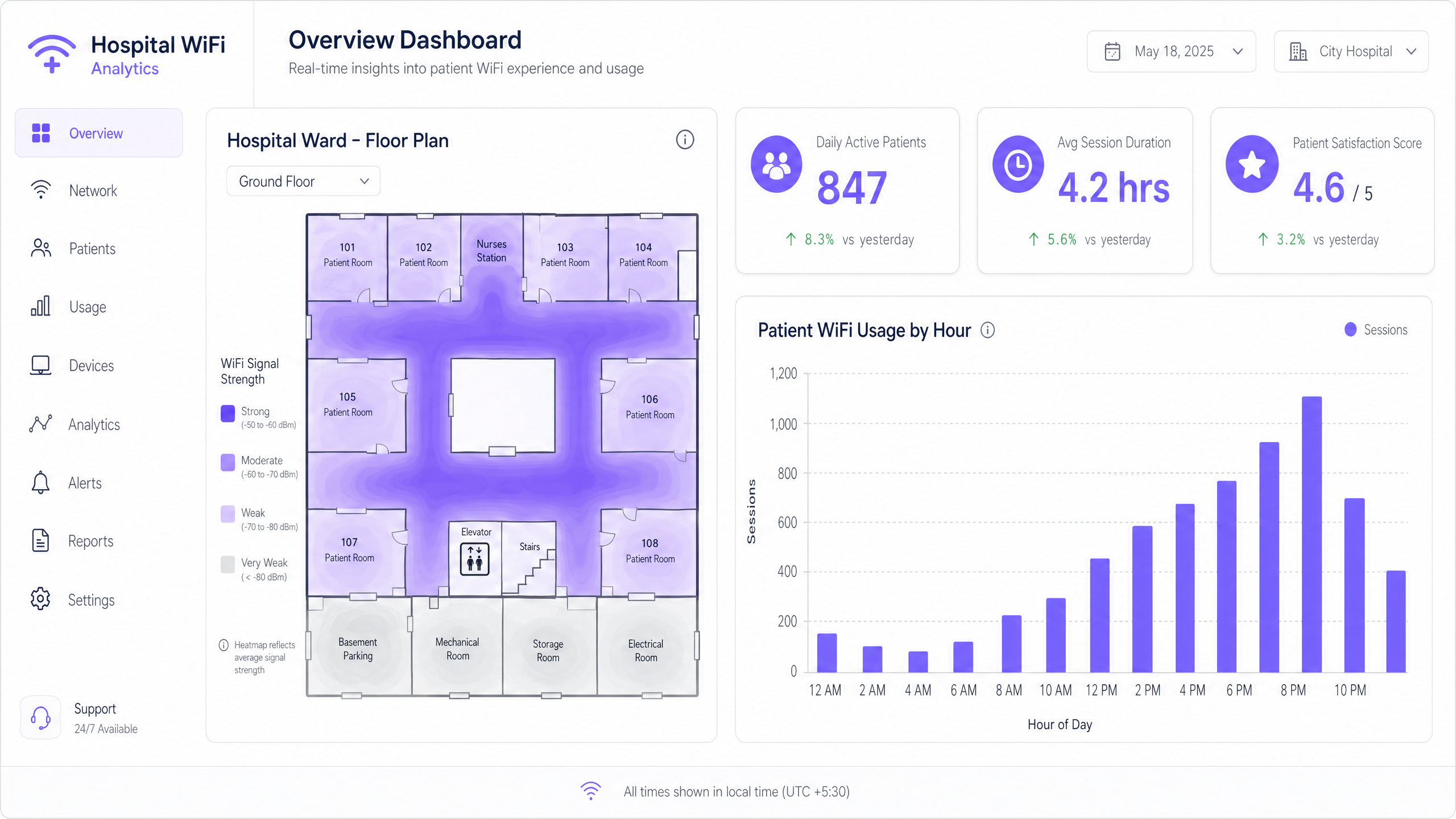
The analytics layer is where patient WiFi transitions from a cost centre to a strategic asset. A properly instrumented network, feeding data into a platform like Purple's WiFi Analytics , provides three categories of actionable intelligence.
Network Performance Monitoring delivers real-time visibility into AP health, channel utilisation, client association rates, and throughput per SSID. This enables proactive fault resolution before patients experience degraded service. Threshold-based alerting on RSSI drops or AP disassociation events is standard practice.
Footfall and Dwell Analytics work by analysing probe request data and association patterns to generate footfall heatmaps showing patient and visitor movement through the facility. This data is directly applicable to staffing decisions — if analytics show a consistent 45-minute queue build-up in the outpatient waiting area between 10:00 and 11:30, that is an operational insight with a direct staffing solution.
Feedback and Satisfaction Loops are enabled through automated post-discharge survey triggers, delivered via the email address captured at captive portal login, providing real-time HCAHPS-relevant data. Response rates for WiFi-triggered surveys consistently outperform paper-based alternatives because the contact is timely and the channel is already established.
Implementation Guide
A phased deployment approach reduces risk and allows for iterative optimisation.
Phase 1 — Discovery and Design (Weeks 1-4)
Commission a professional predictive RF design using the hospital's architectural drawings, followed by an active site survey of any existing infrastructure. Document all sources of RF interference. Define VLAN architecture, firewall policy, and internet uplink strategy. Engage the Information Governance team early to align the captive portal data collection with GDPR and DSPT requirements.
Phase 2 — Infrastructure Deployment (Weeks 5-10)
Deploy and configure switching infrastructure, ensuring PoE++ budget is sufficient for high-density APs. Install APs per the validated RF design. Configure SSIDs, VLAN tagging, and QoS policies. Implement QoS markings to prioritise voice (DSCP EF) and video (DSCP AF41) traffic over best-effort bulk data. This ensures telemedicine sessions and video calls remain stable even under network load.
Phase 3 — Captive Portal and Analytics Integration (Weeks 9-12)
Deploy and brand the captive portal. Integrate with the hospital's CRM or patient engagement platform. Configure the analytics platform with custom venue maps. Establish baseline metrics: daily active users, average session duration, peak concurrent connections, and portal completion rate. Set up automated reporting dashboards for the IT and operations teams.
Phase 4 — Wayfinding Integration (Weeks 12-16)
Integrate indoor positioning with the WiFi infrastructure. Publish the hospital's indoor map to the guest portal or a dedicated patient app. Configure points of interest (wards, departments, cafeteria, car parks). Measure wayfinding adoption rates and correlate with missed appointment data.
Best Practices
| Practice | Rationale | Standard Reference |
|---|---|---|
| Strict VLAN segmentation (clinical vs. guest) | Prevents lateral movement from compromised guest devices | HIPAA Security Rule, NHS DSPT |
| WPA3-SAE encryption | Protects against offline dictionary attacks on guest credentials | IEEE 802.11-2020 |
| Client Isolation on guest SSID | Prevents inter-device communication and data exposure | GDPR Article 25 (Privacy by Design) |
| Band Steering to 5/6 GHz | Reduces congestion and interference from legacy 2.4 GHz devices | Wi-Fi Alliance best practices |
| QoS for voice and video | Maintains call quality under network load | IEEE 802.11e / WMM |
| DNS filtering on guest traffic | Blocks malicious domains and inappropriate content | NCSC network security guidance |
| Dedicated internet uplink for guest traffic | Guarantees clinical network performance is unaffected | NHS DSPT, HIPAA |
| Automated post-discharge feedback surveys | Provides timely, actionable HCAHPS-relevant data | NHS Friends and Family Test guidance |
Troubleshooting & Risk Mitigation
RF Interference from Medical Equipment: Conduct regular spectrum analysis using a dedicated spectrum analyser tool. Legacy nurse call systems and patient monitoring equipment operating on 2.4 GHz are common culprits. The solution is typically a combination of channel reassignment and power reduction on affected APs, combined with a migration plan for the interfering equipment.
Captive Portal Redirect Failures: Modern operating systems use Captive Network Assistant (CNA) probes to detect captive portals. Ensure the portal server responds correctly to HTTP requests to known probe URLs (e.g., connectivitycheck.gstatic.com, captive.apple.com). HTTPS-only portal configurations frequently break CNA detection — maintain an HTTP redirect path even if the portal itself is served over HTTPS.
Coverage Gaps in Shielded Areas: Radiology suites, MRI rooms, and some operating theatres use RF shielding that creates complete signal blackouts. The only solution is to deploy APs inside the shielded space, connected via a penetrating cable entry point. Coordinate with the medical physics team before any cabling work in these areas.
GDPR Compliance Risk: The most common compliance failure is collecting marketing consent as part of the terms of service acceptance, rather than as a separate, explicit opt-in. This is a clear GDPR violation. Audit your captive portal flow to ensure consent for network access and consent for marketing communications are presented as separate, independent choices.
Bandwidth Contention: Without per-user bandwidth policies, a small number of heavy users can degrade the experience for everyone. Implement a per-device rate limit of 5-10 Mbps on the guest SSID. This is sufficient for HD streaming while preventing any single device from monopolising capacity.
ROI & Business Impact
The business case for investing in patient WiFi infrastructure rests on four measurable pillars.
HCAHPS Score Improvement: Patient satisfaction scores directly influence hospital reimbursement rates under value-based care models. Hospitals that have implemented automated WiFi-triggered feedback surveys report response rate improvements of 3-5x over paper-based methods, providing a statistically significant data set for quality improvement programmes.
Reduced Missed Appointments: Indoor wayfinding reduces the rate of patients arriving late or missing appointments due to navigation difficulties. A typical 500-bed hospital with 10% of outpatient appointments affected by navigation issues, at an average appointment cost of £150, represents a significant recoverable revenue opportunity.
Operational Efficiency: Footfall analytics from the WiFi network enable data-driven staffing decisions. Correlating waiting area dwell times with staffing levels allows operations managers to reduce average wait times without increasing headcount — simply by optimising shift patterns against actual demand data.
First-Party Data Asset: Every patient who connects to the guest WiFi and completes the captive portal flow represents a consented first-party data record. For a 500-bed hospital with an average length of stay of 4 days, this generates thousands of new, compliant data records per month — a valuable asset for patient engagement, health promotion communications, and service improvement research.
The Healthcare sector is increasingly recognising that the network is not just IT infrastructure — it is a patient experience platform. Organisations that treat it as such are consistently outperforming peers on satisfaction metrics and operational efficiency.
关键定义
Captive Portal
在用户被授予访问公共 WiFi 网络权限之前向其展示的网页,用于显示服务条款、收集身份验证凭据或同意,并重定向到互联网。
医院访客 WiFi 网络的主要患者接触点。设计质量直接影响门户完成率和数据捕获质量。必须在所有主流移动操作系统上进行测试。
VLAN (Virtual Local Area Network)
在物理交换基础设施中使用 802.1Q 标记创建的逻辑网段,允许不同用户组的流量在第二层隔离,无需单独的物理布线。
对于将患者访客流量与临床 EHR 和管理网络隔离开来至关重要。缺少适当的 VLAN 隔离是医疗 IT 审计中最常见的网络安全发现。
Band Steering
一种无线网络管理技术,鼓励支持双频段的客户端设备关联到拥挤程度较低的 5 GHz 或 6 GHz 射频频段,而不是 2.4 GHz 频段。
在医院环境中特别有价值,因为传统医疗设备会产生严重的 2.4 GHz 干扰。减少拥塞并提高流媒体应用的吞吐量。
Client Isolation
一种无线网络安全功能,防止关联到同一 SSID 的设备在第二层直接相互通信,强制所有流量通过网关。
在医疗访客 SSID 上是强制性的。防止患者设备上的恶意软件扫描或攻击同一网段上的其他设备。还具有关于数据暴露的 GDPR 影响。
WPA3-SAE (Simultaneous Authentication of Equals)
WPA3 认证无线网络中使用的认证协议,用抗离线字典攻击的 Dragonfly 密钥交换替代了 WPA2 的预共享密钥握手。
当前推荐的新 SSID 部署加密标准。即使在开放或轻度安全的网络上也能保护患者凭据和会话数据不被拦截。
RSSI (Received Signal Strength Indicator)
对接收到的无线电信号功率电平的测量,以 dBm(相对于一毫瓦的分贝)表示。负值越大表示信号越弱。
在现场勘察期间用于验证 AP 放置。患者区域的目标是 -67 dBm 或更高。低于 -75 dBm 的值通常会导致连接不稳定和流媒体性能差。
QoS (Quality of Service)
网络流量管理策略,对不同类型的數據包进行分类和优先排序,以确保延迟敏感型应用(语音、视频)获得优于尽力而为流量的优先处理。
对于在高网络利用率期间维持远程医疗通话质量和患者视频通话稳定性至关重要。使用 DSCP 标记实现:语音 EF,视频 AF41。
Location Analytics
从移动设备在场所内移动时产生的 WiFi 探测请求和关联事件中获取移动、停留时间和客流数据的过程。
使医院运营团队能够生成客流热图、识别患者流瓶颈,并根据实际需求数据而非计划假设优化人员配置水平。
HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems)
一项标准化、公开报告的患者对医院护理看法的调查,用于衡量和比较不同医疗机构的患者体验。
WiFi 质量和数字服务可用性与 HCAHPS 沟通和响应性评分的相关性日益增强。WiFi 触发自动调查可提高响应率和数据及时性。
DNS Filtering
一种安全控制,在建立连接之前拦截 DNS 解析请求,并阻止对归类为恶意、不当或违反策略的域的查询。
在所有访客 WiFi 流量的解析器级别应用。为患者网络提供轻量级但有效的保护层,防止恶意软件分发、网络钓鱼和不当内容访问。
应用实例
一家拥有 500 张床位的区域 NHS 医院在其患者 WiFi 在晚间探视时间(18:00-20:00)遭遇严重网络拥塞,导致投诉视频流缓冲和与家人视频通话失败。
- 在高峰时段进行频谱分析,确认问题是射频拥塞还是回程饱和。2. 如果是射频问题:启用频段引导,迫使支持 5 GHz 的设备离开 2.4 GHz 频段;审查 AP 信道分配并降低发射功率以收紧小区边界并减少同频干扰。3. 如果是回程问题:审查高峰时段互联网上行链路利用率——如果共享连接已饱和,则实施流量整形,优先处理实时流量(语音 DSCP EF,视频 DSCP AF41)而非批量下载。4. 在访客 SSID 上实施每设备 8 Mbps 的带宽上限,以确保公平访问。5. 如果在高峰时段每 AP 客户端数量超过 30,则在最密集的病房部署额外 AP。6. 审查特定病房的分析仪表盘,这些病房产生的投诉最多——问题很少在整个设施内均匀分布。
一家私立医院集团正在部署新的门诊诊所,希望使用访客 WiFi Captive Portal 收集患者数据用于诊后反馈调查和营销通信,同时确保与包含 EHR 数据的临床网络严格隔离。
- 为访客 SSID 创建专用 VLAN(例如 VLAN 100),使用单独的 DHCP 作用域且不与临床 VLAN 建立路由邻接关系。2. 通过单独的防火墙区域将所有访客流量路由到专用互联网上行链路——不要使用保护临床系统的同一边界防火墙。3. 在访客 SSID 上启用 Client Isolation。4. 设计 Captive Portal 时使用两个独立的同意复选框:一个用于接受网络服务条款(访问所必需),另一个用于选择加入营销通信(可选,明确标注)。这是 GDPR 第 7 条的要求——营销同意必须自由给予,并与服务条件分开。5. 将门户与 Purple 的 Guest WiFi 平台集成,以将获得同意的数据捕获为兼容 CRM 的格式。6. 配置自动诊后调查触发器在患者会话结束后 24 小时触发。7. 在访客 VLAN 上实施 DNS 过滤以阻止恶意域。
练习题
Q1. 一位医院管理员提议使用访客 WiFi 网络来追踪昂贵的移动医疗设备(输液泵、便携式心电监护仪)的实时位置。作为 IT 总监,您如何回应,您推荐什么替代方案?
提示:考虑访客与临床基础设施之间的架构隔离,以及临床环境中资产追踪的可靠性要求。
查看标准答案
我会建议不要使用访客 WiFi 网络进行临床资产追踪,原因有二。首先,访客 SSID 在架构上与临床系统隔离——任何资产追踪数据都需要穿越防火墙边界才能到达临床管理系统,这会引入不必要的复杂性和潜在安全风险。其次,访客 WiFi 的位置精度(使用 RSSI 三角测量通常为 5-15 米)不足以在临床环境中实现可靠的房间级资产追踪。推荐的替代方案是使用有源 BLE 标签的专用 RTLS,并在每个房间安装专用 BLE 读取器。这提供了亚米级精度,独立于访客网络运行,并直接与临床资产管理系统集成。BLE 基础设施通常可以与 WiFi AP 共享相同的物理布线,降低部署成本。
Q2. 在部署后审计中,您发现医院的 Captive Portal 只提供一个复选框,上面写着:'我接受服务条款并同意接收来自医院的通信。' 存在什么合规风险,如何修复?
提示:考虑 GDPR 第 7 条对有效同意的要求,特别是同意被视为自由给予的条件。
查看标准答案
这明显违反了 GDPR 第 7 条。营销通信的同意必须自由给予,这意味着不能将其与网络访问同意捆绑作为服务条件。修复方法是将 Captive Portal 拆分为两个不同的同意机制:(1) 强制接受网络服务条款(访问所必需),(2) 一个单独的、可选的选择加入营销通信复选框,明确标注且默认未选中。对在捆绑同意下捕获的任何现有记录,应与数据保护官进行审查——在重新获得同意之前,可能需将其视为营销用途未经同意。
Q3. 一家现有医院正在增建一座 200 张床位的新肿瘤科大楼。项目经理询问是否可以直接扩展现有访客 WiFi 基础设施来覆盖新大楼。在提出建议之前,您会问哪些问题?
提示:在假设现有基础设施可扩展之前,考虑容量规划、回程以及新建筑结构的特定射频挑战。
查看标准答案
在提出任何建议之前,我会问:(1) 现有回程上行链路在高峰时段的当前利用率如何?若已超过 70%,增加 200 张床位将导致争用。(2) 新大楼的建筑规格——具体来说,是否有任何铅衬房间或钢筋混凝土楼板需要 AP 安装在屏蔽空间内?(3) 现有基础设施在高峰时段每 AP 的客户端数量是多少?若现有 AP 已处理超过 40 个客户端,即使增加额外设备,现有 AP 硬件也可能不够。(4) 现有交换基础设施是否支持 PoE++,还是需要新交换机?(5) 是否已针对新大楼的建筑图纸进行过预测性射频设计?若没有正式容量评估和预测设计,我不会建议仅简单地扩展现有基础设施。
继续阅读本系列
第一方数据营销:企业综合指南
本指南阐述了如何利用企业级宾客 WiFi 网络构建强大的第一方数据营销策略。它涵盖了通过 Captive Portal 安全捕获数据的技术架构、符合 GDPR 的合规同意工作流、CRM 集成模式以及自动化营销活动的部署。酒店、零售、活动和公共部门环境的场馆运营商将找到实用的指导,将盲目访问的访客转化为高价值的自有营销受众。
客户数据管理平台:面向企业的全面指南
本指南阐述了场所运营商如何部署客户数据管理平台来统一零散的访客数据。内容涵盖技术架构、集成策略,以及 Guest WiFi 在构建第一方数据画像中的关键作用。
衡量客用 WiFi 和位置分析的商业投资回报率
本指南为衡量客用 WiFi 和位置分析的商业投资回报率 (ROI) 提供了技术和运营框架。它详细介绍了如何通过零售、酒店和公共场所的停留时间提升、运营效率以及第一方数据采集,来计算硬件投资的价值。IT 经理、网络架构师、CTO 和场所运营总监将获得具体的衡量框架、真实案例研究和合规性指南,以证明并最大化其 WiFi 投资。